Notes

DEFINITION
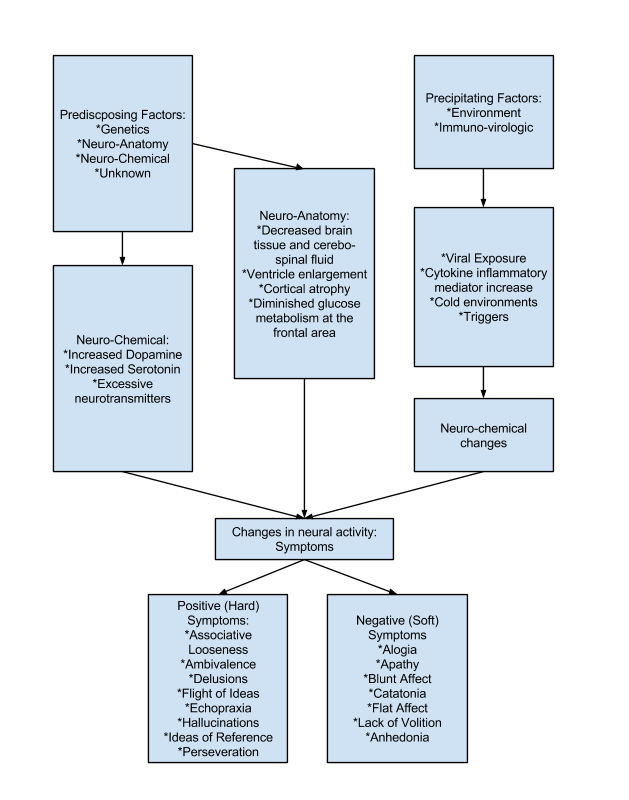
Schizophrenia is an extremely complex mental disorder: in fact it is probably many illnesses masquerading as one. A biochemical imbalance in the brain is believed to cause symptoms. Recent research reveals that schizophrenia may be a result of faulty neuronal development in the fetal brain, which develops into full-blown illness in late adolescence or early adulthood.
Schizophrenia causes distorted and bizarre thoughts, perceptions, emotions, movement, and behavior. It cannot be defined as a single illness;
rather thought as a syndrome or disease process with many different varieties and symptoms. It is usually diagnosed in late adolescence or early adulthood. Rarely does it manifest in childhood. The peak incidence of onset is 15 to 25 years of age for men and 25 to 35 years of age for women.
The symptoms of schizophrenia are categorized into two major categories, the positive or hard symptoms which include delusion, hallucinations, and grossly disorganized thinking, speech, and behavior, and negative or soft symptoms as flat affect, lack of volition, and social withdrawal or discomfort. Medication treatment can control the positive symptoms but frequently the negative symptoms persist after positive symptoms have abated. The persistence of these negative symptoms over time presents a major barrier to recovery and improved the functioning of client’s daily life.
PATHOPHYSIOLOGY
TYPES OF SCHIZOPHRENIA:
The diagnosis is made according to the client’s predominant symptoms:
- Schizophrenia, paranoid type is characterized by persecutory (feeling victimized or spied on) or grandiose delusions, hallucinations, and occasionally, excessively religiosity (delusional focus) or hostile and aggressive behavior.
- Schizophrenia, disorganized type is characterized by grossly inappropriate or flat affect, incoherence, loose associations, and extremely disorganized behavior.
- Schizophrenia, catatonic type is characterized by marked psychomotor disturbance, either motionless or excessive motor activity. Motor immobility may be manifested by catalepsy (waxy flexibility) or stupor.
- Schizophrenia, undifferentiated type is characterized by mixed schizophrenic symptoms (of other types) along with disturbances of thought, affect, and behavior.
- Schizophrenia, residual type is characterized by at least one previous, though not a current, episode, social withdrawal, flat affect and looseness of associations.
Paranoid Schizophrenia
- Is characterized by persecutory or grandiose delusional thought content and, possibly, delusional jealousy.
- Some patients also have gender identity problems, such as fears of being thought of as homosexual or of being approached by homosexuals.
- Stress may worsen the patient’s symptoms.
- Paranoid schizophrenia may cause only minimal impairment in the patient’s level of functioning – as long as he doesn’t act on delusional thoughts.
- Although patients with paranoid schizophrenia may experience frequent auditory hallucinations (usually related to a single theme), they typically lack some of the symptoms of other schizophrenia subtypes – notably, incoherent, loose associations, flat or grossly inappropriate affect, and catatonic or grossly disorganized behavior.
- Tend to be less severely disabled than other schizophrenia.
- Those with late onset of disease and good pre-illness functioning (ironically, the very patients who have the best prognosis) are at the greatest risk for suicide.
Signs and Symptoms
- Persecutory or grandiose delusional thoughts
- Auditory hallucinations
- Unfocused anxiety
- Anger
- Tendency to argue
- Stilted formality or intensity when interacting with others
- Violent behavior
Diagnosis
- Ruling out other causes of the patient’s symptoms.
- Meeting the DSM-IV-TR criteria.
Treatment
- Antipsychotic drug therapy.
- Psychosocial therapies and rehabilitation, including group and individual psychotherapy.
Nursing Interventions
- Build trust, and be honest and dependable, don’t threaten or make promises you can’t fulfill.
- Be aware that brief patient contacts may be most useful initially.
- When the patient is newly admitted, minimize his contact with the staff.
- Don’t touch the patient without telling him first exactly what you’re going to be doing and before obtaining his permission to touch him.
- Approach him in a calm, unhurried manner.
- Avoid crowding him physically or psychologically; he may strike out to protect himself.
- Respond neutrally to his condescending remarks; don’t let him put you on the defensive, and don’t take his remarks personally.
- If he tells you to leave him alone, do leave- but make sure you return soon.
- Set limits firmly but without anger, avoid a punitive attitude.
- Be flexible, giving the patient as much control as possible.
- Consider postponing procedures that require physical contact with hospital personnel if the patient becomes suspicious or agitated.
- If the patient has auditory hallucinations, explore the content of the hallucinations (what voices are saying to him, whether he thinks he must do what they command) tell him you don’t hear voices, but you know they’re real to him.
Disorganized Schizophrenia
- Is marked by incoherent, disorganized speech and behaviors and by blunted or inappropriate affect.
- May have fragmented hallucinations and delusions with no coherent theme.
- Usually includes extreme social impairment.
- This type of schizophrenia may start early and insidiously, with no significant remissions.
Signs and Symptoms
- Incoherent, disorganized speech, with markedly loose associations.
- Grossly disorganized behavior.
- Blunted, silly, superficial, or inappropriate affect.
- Grimacing
- Hypochondriacal complaints.
- Extreme social withdrawal.
Diagnosis
- Ruling out other causes of the patients symptoms.
- Meeting the DSM-IV-TR criteria.
Treatment
- Treatments described for other types of schizophrenia.
- Antipsychotic drugs and psychotherapy.
Nursing Interventions
- Spend time with the patient even if he’s mute and unresponsive, to promote reassurance and support.
- Remember that, despite appearances, the patient is acutely aware of his environment, assume the patient can hear – speak to him directly and don’t talk about him in his presence.
- Emphasize reality during all patient contacts, to reduce distorted perceptions (for example, say, “The leaves on the trees are turning colors and the air is cooler, It’s fall”)
- Verbalize for the patient the message that his behavior seems to convey, encourage him to do the same.
- Tell the patient directly, specifically, and concisely what needs to be done; don’t give him choice (for example, say, “It’s time to go for a walk, lets go.”)
- Assess for signs and symptoms of physical illness; keep in mind that if he’s mute he won’t complain of pain or physical symptoms.
- Remember that if he’s in bizarre posture, he may be at risk for pressure ulcers or decreased circulation.
- Provide range-of-motion exercises.
- Encourage to ambulate every 2 hours.
- During periods of hyperactivity, try to prevent him from experiencing physical exhaustion and injury.
- As appropriate, meet his needs for adequate food, fluid, exercise, and elimination; follow orders with respect to nutrition, urinary catheterization, and enema use.
- Stay alert for violent outbursts; if these occur, get help promptly to intervene safely for yourself, the patient, and others.
Catatonic Schizophrenia
- Is a rare disease form in which the patient tends to remain in a fixed stupor or position for long periods, periodically yielding to brief spurts of extreme excitement.
- Many catatonic schizophrenia have an increased potential for destructive, violent behavior when agitated.
Signs and Symptoms
- Remaining mute; refusal to move about or tend to personal needs.
- Exhibiting bizarre mannerisms, such as facial grimacing and sucking mouth movements.
- Rapid swing between stupor and excitement (extreme psychomotor agitation with excessive, senseless, or incoherent shouting or talking).
- Bizarre posture such as holding the body (especially the arms and legs) rigidly in one position for a long time.
- Diminished sensitivity to painful stimuli.
- Echolalia (repeating words or phrases spoken by others).
- Echopraxia (imitating other’s movements).
Diagnosis
- Ruling out other possible causes of the patient’s symptoms.
- Meeting the DSM-IV-TR criteria.
Treatment
- ECT and benzodiazepines (such as diazepam or lorazepam) for catatonic schizophrenia.
- Avoiding conventional antipsychotic drugs (they may worsen catatonic symptoms).
- Investigating atypical antipsychotic drugs to treat catatonic schizophrenia (requires further evaluation).
Nursing Interventions
- Spend time with the patient even if he’s mute and unresponsive, to promote reassurance and support.
- Remember that, despite appearances, the patient is acutely aware of his environment, assume the patient can hear – speak to him directly and don’t talk about him in his presence.
- Emphasize reality during all patient contacts, to reduce distorted perceptions (for example, say, “The leaves on the trees are turning colors and the air is cooler, It’s fall”)
- Verbalize for the patient the message that his behavior seems to convey, encourage him to do the same.
- Tell the patient directly, specifically, and concisely what needs to be done; don’t give him choice (for example, say, “It’s time to go for a walk, lets go.”)
- Assess for signs and symptoms of physical illness; keep in mind that if he’s mute he won’t complain of pain or physical symptoms.
- Remember that if he’s in bizarre posture, he may be at risk for pressure ulcers or decreased circulation.
- Provide range-of-motion exercises.
- Encourage to ambulate every 2 hours.
- During periods of hyperactivity, try to prevent him from experiencing physical exhaustion and injury.
- As appropriate, meet his needs for adequate food, fluid, exercise, and elimination; follow orders with respect to nutrition, urinary catheterization, and enema use.
- Stay alert for violent outbursts; if these occur, get help promptly to intervene safely for yourself, the patient, and others.
DIAGNOSTIC TEST:
- Clinical diagnosis is developed on historical information and thorough mental status examination.
- No laboratory findings have been identified that are diagnostic of schizophrenia.
- Routine battery of laboratory test may be useful in ruling out possible organic etiologies, including CBC, urinalysis, liver function tests, thyroid function test, RPR, HIV test, serum ceruloplasmin ( rules out an inherited disease, wilson’s disease, in which the body retains excessive amounts of copper), PET scan, CT scan, and MRI.
- Rating scale assessment:
-
- Scale for the assessment of negative symptoms.
- Scale for the assessment of positive symptoms.
- Brief psychiatric rating scale
TREATMENTS AND MEDICATIONS:
Currently, there is no method for preventing schizophrenia and there is no cure. Minimizing the impact of disease depends mainly on early diagnosis and, appropriate pharmacological and psycho-social treatments. Hospitalization may be required to stabilize ill persons during an acute episode. The need for hospitalization will depend on the severity of the episode. Mild or moderate episodes may be appropriately addressed by intense outpatient treatment. A person with schizophrenia should leave the hospital or outpatient facility with a treatment plan that will minimize symptoms and maximize quality of life.
A comprehensive treatment program can include:
- Antipsychotic medication
- Education & support, for both ill individuals and families
- Social skills training
- Rehabilitation to improve activities of daily living
- Vocational and recreational support
- Cognitive therapy
Medication is one of the cornerstones of treatment. Once the acute stage of a psychotic episode has passed, most people with schizophrenia will need to take medicine indefinitely. This is because vulnerability to psychosis doesn’t go away, even though some or all of the symptoms do. In North America, atypical or second generation antipsychotic medications are the most widely used. However, there are many first-generation antipsychotic medications available that may still be prescribed. A doctor will prescribe the medication that is the most effective for the ill individual
Another important part of treatment is psychosocial programs and initiatives. Combined with medication, they can help ill individuals effectively manage their disorder. Talking with your treatment team will ensure you are aware of all available programs and medications.
In addition, persons living with schizophrenia may have access to or qualify for income support programs/initiatives, supportive housing, and/or skills development programs, designed to promote integration and recovery.
Practice Exam
Nursing Care Plan
Disturbed Sensory Perception: Auditory/Visual
Disturbed Sensory Perception: Change in the amount or patterning of incoming stimuli accompanied by a diminished, exaggerated, distorted or impaired response to such stimuli.
May be related to
- Altered sensory perception.
- Altered sensory reception; transmission or integration.
- Biochemical factors such as manifested by inability to concentrate.
- Chemical alterations (e.g., medications, electrolyte imbalances).
- Neurologic/biochemical changes.
- Psychologic stress.
Possibly evidenced by
- Altered communication pattern.
- Auditory distortions.
- Change in a problem-solving pattern.
- Disorientation to person/place/time.
- Frequent blinking of the eyes and grimacing.
- Hallucinations.
- Inappropriate responses.
- Mumbling to self, talking or laughing to self.
- Reported or measured change in sensory acuity.
- Tilting the head as if listening to someone.
Desired Outcomes
- Patient will learn ways to refrain from responding to hallucinations.
- Patient will state three symptoms they recognize when their stress levels are high.
- Patient will state that the voices are no longer threatening, nor do they interfere with his or her life.
- Patient will state, using a scale from 1 to 10, that “the voices” are less frequent and threatening when aided by medication and nursing intervention.
- Patient will maintain role performance.
- Patient will maintain social relationships.
- Patient will monitor intensity of anxiety.
- Patient will identify two stressful events that trigger hallucinations..
- Patient will identify to personal interventions that decrease or lower the intensity or frequency of hallucinations (e.g, listening to music, wearing headphones, reading out loud, jogging, socializing).
- Patient will demonstrate one stress reduction technique.
- Patient will demonstrate techniques that help distract him or her from the voices.
| Nursing Interventions | Rationale |
|---|---|
| Accept the fact that the voices are real to the client, but explain that you do not hear the voices. Refer to the voices as “your voices” or “voices that you hear”. | Validating that your reality does not include voices can help client cast “doubt” on the validity of his or her voices. |
| Be alert for signs of increasing fear, anxiety or agitation. | Might herald hallucinatory activity, which can be very frightening to client, and client might act upon command hallucinations (harm self or others). |
| Explore how the hallucinations are experienced by the client. | Exploring the hallucinations and sharing the experience can help give the person a sense of power that he or she might be able to manage the hallucinatory voices. |
| Help the client to identify the needs that might underlie the hallucination. What other ways can these needs be met? | Hallucinations might reflect needs for:
|
| Help client to identify times that times that the hallucinations are most prevalent and frightening. | Helps both nurse and client identify situations and times that might be most anxiety producing and threatening to the client. |
If voices are telling the client to harm self or others, take necessary environmental precautions.
Clearly document what client says and if he/she is a threat to others, document who was contacted and notified (use agency protocol as a guide). |
People often obey hallucinatory commands to kill self or others. Early assessment and intervention might save lives. |
| Stay with clients when they are starting to hallucinate, and direct them to tell the “voices they hear” to go away. Repeat often in a matter-of-fact manner. | Client can sometimes learn to push voices aside when given repeated instructions. especially within the framework of a trusting relationship. |
| Decrease environmental stimuli when possible (low noise, minimal activity). | Decrease potential for anxiety that might trigger hallucinations. Helps calm client. |
| Intervene with one-on-one, seclusion, or PRN medication (As ordered) when appropriate. | Intervene before anxiety begins to escalate. If the client is already out of control, use chemical or physical restraints following unit protocols. |
| Keep to simple, basic, reality-based topics of conversation. Help client focus on one idea at a time. | Client’ thinking might be confused and disorganized; this intervention helps client focus and comprehend reality-based issues. |
| Work with the client to find which activities help reduce anxiety and distract the client from a hallucinatory material. Practice new skills with the client. | If clients’ stress triggers hallucinatory activity, they might be more motivated to find ways to remove themselves from a stressful environment or try distraction techniques. |
| Engage client in reality-based activities such as card playing, writing, drawing, doing simple arts and crafts or listening to music. | Redirecting client’s energies to acceptable activities can decrease the possibility of acting on hallucinations and help distract from voices. |
Disturbed Thought Process
Disturbed Thought Process: Disruption in cognitive operations and activities.
May be related to
- Chemical alterations (e.g., medications, electrolyte imbalances).
- Inadequate support systems.
- Overwhelming stressful life events.
- Possibility of a hereditary factor.
- Panic level of anxiety.
- Repressed fears.
Possibly evidenced by
- Delusions.
- Inaccurate interpretation of environment.
- Inappropriate non-reality-based thinking.
- Memory deficit/problems.
- Self-centeredness.
Desired Outcomes
- Patient will verbalize recognition of delusional thoughts if they persist.
- Patient will perceive environment correctly.
- Patient will demonstrate satisfying relationships with real people.
- Patient will demonstrate decrease anxiety level.
- Patient will refrain from acting on delusional thinking.
- Patient will develop trust in at least one staff member within 1 week.
- Patient will sustain attention and concentration to complete task or activities.
- Patient will state that the “thoughts” are less intense and less frequent with the help of the medications and nursing interventions.
- Patient will talk about concrete happenings in the environment without talking about delusions for 5 minutes.
- Patient will demonstrate two effective coping skills that minimize delusional thoughts.
- Patient will be free from delusions or demonstrate the ability to function without responding to persistent delusional thoughts.
| Nursing Interventions | Rationale |
|---|---|
| Attempt to understand the significance of these beliefs to the client at the time of their presentation. | Important clues to underlying fears and issues can be found in the client’s seemingly illogical fantasies. |
| Recognizes the client’s delusions as the client’s perception of the environment. | Recognizing the client’s perception can help you understand the feelings he or she is experiencing. |
Identify feelings related to delusions. For example:
|
When people believe that they are understood, anxiety might lessen. |
| Explain the procedures and try to be sure the client understand the procedures before carrying them out. | When the client has full knowledge of procedures, he or she is less likely to feel tricked by the staff. |
| Interact with clients on the basis of things in the environment. Try to distract client from their delusions by engaging in reality-based activities (e.g., card games, simple arts and crafts projects etc). | When thinking is focused on reality-based activities, the client is free of delusional thinking during that time. Helps focus attention externally. |
| Do not touch the client; use gestures carefully. | Suspicious clients might misinterpret touch as either aggressive or sexual in nature and might interpret it as threatening gesture. People who are psychotic need a lot of personal space. |
| Initially do not argue with the client’s beliefs or try to convince the client that the delusions are false and unreal. | Arguing will only increase client’s defensive position, thereby reinforcing false beliefs. This will result in the client feeling even more isolated and misunderstood. |
Encourage healthy habits to optimize functioning:
|
All are vital to help keep the client in remission. |
| Show empathy regarding the client’s feelings; reassure the client of your presence and acceptance. | The client’s delusion can be distressing. Empathy conveys your caring, interest and acceptance of the client. |
Teach client coping skills that minimize “worrying” thoughts. Coping skills include:
|
When client is ready, teach strategies client can do alone. |
| Utilize safety measures to protect clients or others, if the client believe they need to protect themselves against a specific person. Precautions are needed. | During acute phase, client’s delusional thinking might dictate to them that they might have to hurt others or self in order to be safe. External controls might be needed. |
Defensive Coping
Defensive Coping: Repeated projection of falsely positive self-evaluation based on a self-protective pattern that defends against underlying perceived threats to positive self-regard.
May be related to
- Perceived lack of self-efficacy/vulnerability.
- Perceived threat to self.
- Suspicions of the motives of others.
Possibly evidenced by
- Denial of obvious problems.
- Difficulty in reality testing of perceptions.
- Difficulty establishing/maintaining relationships.
- False beliefs about the intention of others.
- Fearful.
- Grandiosity.
- Hostile laughter or ridicule of others.
- Hostility, aggression, or homicidal ideation.
- Projection of blame/responsibility.
- Rationalization of failures.
- Superior attitude towards others.
Desired Outcomes
- Patient will avoid high-risk environments and situations.
- Patient will interact with others appropriately.
- Patient will maintain medical compliance.
- Patient will identify one action that helps client feel more in control of his or her life.
- Patient will demonstrate two newly learned constructive ways to deal with stress and feeling of powerlessness.
- Patient will demonstrate learn the ability to remove himself or herself from situations when anxiety begins to increase with the aid of medications and nursing interventions.
- Patient will demonstrate decreased suspicious behaviors regarding with the interaction with others.
- Patient will be able to apply a variety of stress/anxiety-reducing techniques on their own.
- Patient will acknowledge that medications will lower suspiciousness.
- Patient will state that he/she feels safe and more in control with interactions with environment/family/work/social gatherings.
| Nursing Interventions | Rationale |
|---|---|
| Explain to client what you are going to do before you do it. | Prepares the client beforehand and minimizes misinterpreting your intent as hostile or aggressive. |
| Assess and observe clients regularly for signs of increasing anxiety and hostility. | Intervene before client loses control. |
| Use a nonjudgemental, respectful, and neutral approach with the client. | There is less chance for a suspicious client to misinterpret intent or meaning if content is neutral and approach is respectful and non-judgemental. |
| Use clear and simple language when communicating with a suspicious client. | Minimize the opportunity for miscommunication and misconstruing the meaning of the message. |
| Diffuse angry verbal attacks with a non defensive stand. | When staff become defensive, anger escalates for both client and staff. a non-defensive and non-judgemental attitude provides an atmosphere in which feelings can be explored more easily. |
| Set limits in a clear matter-of-fact way, using a calm tone. Giving threatening remarks to Jeremy is unacceptable. We can talk more about the proper ways in dealing with your feelings. | Calm and neutral approach may diffuse escalation of anger. Offer an alternative to verbal abuse by finding appropriate ways to deal with feelings. |
| Be honest and consistent with client regarding expectations and enforcing rules. | Suspicious people are quick to discern honesty. Honesty and consistency provide an atmosphere in which trust can grow. |
| Maintain low level of stimuli and enhance a non-threatening environment (avoid groups). | Noisy environments might be perceived as threatening. |
Be aware of client’s tendency to have ideas of reference; do not do things in front of client that can be misinterpreted:
|
Suspicious clients will automatically think that they are the target of the interaction and interpret it in a negative manner (e.g., you are laughing or whispering about them). |
| Initially, provide solitary, noncompetitive activities that take some concentration. Later a game with one or more client that takes concentration (e.g., chess checkers, thoughtful card games such as ridge or rummy). | If a client is suspicious of others, solitary activities are the best. Concentrating on environmental stimuli minimizes paranoid rumination. |
| Provide verbal/physical limits when client’s hostile behavior escalates: We cannot allow you to verbally attack someone here. If you cant held/control yourself, we are here in order to help you. | Often verbal limits are effective in helping a client gain self control. |
Interrupted Family Process
Interrupted Family Process: Change in family relationships and/or functioning.
May be related to
- Developmental crisis or transition.
- Family role shift.
- Physical or mental disorder of a family member.
- Shift in health status of a family member.
- Situational crisis or transistion.
Possibly evidenced by
- Changes in expression of conflict in family.
- Changes in communication patterns.
- Changes in mutual support.
- Changes in participation in decision making.
- Changes in participation in problem solving.
- Changes in stress reduction behavior.
- Knowledge deficit regarding community and health care support.
- Knowledge deficit regarding the disease and what is happening with ill family member (might believe client is more capable than they are).
- Inability to meet the needs of family and significant others (physical, emotional, spiritual).
Desired Outcomes
- Family and/or significant others will recount in some detail the early signs and symptoms of relapse in their ill family member, and know whom to contact in case.
- Family and/or significant others will state and have written information identifying the signs of potential relapse and whom to contact before discharge.
- Family and/or significant others will state that they have received needed support from community and agency resources that offer education, support, coping skills training, and/or social network development (psychoeducational approach).
- Family and/or significant others will state what medications can do for their ill family member, the side effects and toxic effects of the drugs, and the need for adherence to medication at least 2 to 3 days before discharge.
- Family and/or significant others will name and have a complete list of community supports for ill family members and supports for all members of the family at least 2 days before the discharge.
- Family and/or significant others will attend at least one family support group (single family, multiple family) within 4 days from onset of acute episode.
- Family and/or significant others will be included in the discharge planning along with the client.
- Family and/or significant others will meet with nurse/physician/social worker the first day of hospitalization and begin to learn about neurologic/biochemical disease, treatment, and community resources.
- Family and/or significant others will problem-solve, with the nurse, two concrete situations within the family that all would like to discharge.
- Family and/or significant others will recount in some detail the early signs and symptoms of relapse in their ill family member, and know whom to contact.
- Family and/or significant others will demonstrate problem-solving skills for handling tensions and misunderstanding within the family member.
- Family and/or significant others will have access to family/multiple family support groups and psychoeducational training.
- Family and/or significant others will know of at least two contact people when they suspect potential relapse.
- Family and/or significant others will discuss the disease (schizophrenia) knowledgeably:
- Know about community resources (e.g., help with self care activities, private respite).
- Support the ill family member in maintaining optimum health.
- Understand the need for medical adherence.
| Nursing Interventions | Rationale |
|---|---|
| Assess the family members’ current level of knowledge about the disease and medications used to treat the disease. | Family might have misconceptions and misinformation about schizophrenia and treatment, or no knowledge at all. Teach client’s and family’s level of understanding and readiness to learn. |
| Inform the client family in clear, simple terms about psychopharmacologic therapy: dose, duration, indication, side effects, and toxic effects. Written information should be given to client and family members as well. | Understanding of the disease and the treatment of the disease encourages greater family support and client adherence. |
| Identify family’s ability to cope (e.g., experience of loss, caregiver burden, needed supports). | Family’s need must be addressed to stabilize family unit. |
| Teach the client and family the warning symptoms of relapse. | Rapid recognition of early warning symptoms can help ward off potential relapse when immediate medical attention is sought. |
| Provide information on disease and treatment strategies at family’s level of understanding. | Meet family members’ needs for information. |
| Provide an opportunity for the family to discuss feelings related to ill family member and identify their immediate concerns. | Nurses and staff can best intervene when they understand the family’s experience and needs. |
| Provide information on client and family community resources for the client and family after discharge: day hospitals, support groups, organizations,psychoeducational programs, community respite centers (small homes), etc. | Schizophrenia is an overwhelming disease for both the client and the family. Groups, support groups, and psychoeducational centers can help:
|
Impaired Verbal Communication
Impaired Verbal Communication: decreased, reduced, delayed, or absent ability to receive, process, transmit, or use a system of symbols.
May be related to
- Altered perceptions.
- Biochemical alterations in the brain of certain neurotransmitters.
- Psychological barriers (lack of stimuli).
- Side effects of medication.
Possibly evidenced by
- Difficulty communicating thoughts verbally.
- Difficulty in discerning and maintaining the usual communication pattern.
- Disturbances in cognitive associations (e.g., perseveration, derailment, poverty of speech, tangentiality, illogicality, neologism, and thought blocking).
- Inappropriate verbalization.
Desired Outcomes
- Patient will express thoughts and feelings in a coherent, logical, goal-directed manner.
- Patient will demonstrate reality-based thought processes in verbal communication.
- Patient will spend time with one or two other people in structured activity neutral topics.
- Patient will spend two to three 5-minute sessions with nurse sharing observations in the environment within 3 days.
- Patient will be able to communicate in a manner that can be understood by others with the help of medication and attentive listening by the time of discharge.
- Patient will learn one or two diversionary tactics that work for him/her to decrease anxiety, hence improving the ability to think clearly and speak more logically.
| Nursing Interventions | Rationale |
|---|---|
| Assess if incoherence in speech is chronic or if it is more sudden, as in an exacerbation of symptoms. | Establishing a baseline facilitates the establishment of realistic goals, the foundation for planning effective care. |
| Identify the duration of the psychotic medication of the client. | Therapeutic levels of an antipsychotic aids clear thinking and diminishes derailment or looseness of association. |
| Keep voice in a low manner and speak slowly as much as possible. | High-pitched/loud tone of voice can elevate anxiety levels while slow speaking aids understanding. |
| Keep environment calm, quiet and as free of stimuli as possible. | Keep anxiety from escalating and increasing confusion and hallucinations/delusions. |
| Plan short, frequent periods with a client throughout the day. | Short periods are less stressful, and periodic meetings give a client a chance to develop familiarity and safety. |
| Use clear or simple words, and keep directions simple as well. | Client might have difficulty processing even simple sentences. |
| Use simple, concrete, and literal explanations. | Minimizes misunderstanding and/or incorporating those misunderstandings into delusional systems. |
| Focus on and direct client’s attention to concrete things in the environment. | Helps draw focus away from delusions and focus on reality-based things. |
| Look for themes in what is said, even though spoken words appear incoherent (e.g., fearful, sadness, guilt). | Often client’s choice of words is symbolic of feelings. |
| When you do not understand a client, let him/her know you are having difficulty understanding. | Pretending to understand limits your credibility in the eyes of your client and lessens the potential for trust. |
When client is ready, introduce strategies that can minimize anxiety and lower voices and “worrying” thoughts, teach client to do the following:
|
Helping client to use tactics to lower anxiety can help enhance functional speech. |
| Use therapeutic techniques (clarifying feelings when speech and thoughts are disorganized) to try to understand client’s concerns. | Even if the words are hard to understand, try getting to the feelings behind them. |
Impaired Social Interaction
Impaired Social Interaction: The state in which an individual participates in an insufficient or excessive quantity or ineffective quality of social exchange.
May be related to
- Difficulty with communication.
- Difficulty with concentration.
- Exaggerated response to alerting stimuli.
- Feeling threatened in social situations.
- Impaired thought processes (delusions or hallucinations).
- Inadequate emotional responses.
- Self concept disturbance (verbalization of negative feelings about self).
Possibly evidenced by
- Appears upset, agitated, or anxious when others come too close in contact or try to engage him/her in an activity.
- Dysfunctional interaction with others/peers.
- Inappropriate emotional response.
- Observed use of unsuccessful social interactions behaviors.
- Spends time alone by self.
- Unable to make eye contact, or initiate or respond to social advances of others.
- Verbalized or observed discomfort in social situations.
Desired Outcomes
- Patient will attend one structured group activity within 5-7 days.
- Patient will seek out supportive social contacts.
- Patient will improve social interaction with family, friends, and neighbors.
- Patient will use appropriate social skills in interactions.
- Patient will engage in one activity with a nurse by the end of the day.
- Patient will maintain an interaction with another client while doing an activity (e.g., simple board game, drawing).
- Patient will demonstrate interest to start coping skills training when ready for learning.
- Patient will engage in one or two activities with minimal encouragement from nurse or family members.
- Patient will state that he or she is comfortable in at least three structured activities that are goal directed.
- Patient will use appropriate skills to initiate and maintain an interaction.
| Nursing Interventions | Rationale |
|---|---|
| Assess if the medication has reached therapeutic levels. | Many of the positive symptoms of schizophrenia (hallucinations, delusions, racing thoughts) will subside with medications, which will facilitate interactions. |
| Identify with client symptoms he experiences when he or she begins to feel anxious around others. | Increased anxiety can intensify agitation, aggressiveness, and suspiciousness. |
| Keep client in an environment as free of stimuli (loud noises, crowding) as possible. | Client might respond to noises and crowding with agitation, anxiety, and increased inability to concentrate on outside events. |
| Avoid touching the client. | Touch by an unknown person can be misinterpreted as a sexual or threatening gesture. This particularly true for a paranoid client. |
| Ensure that the goals set are realistic; whether in the hospital or community. | Avoids pressure on the client and sense of failure on part of nurse/family. This sense of failure can lead to mutual withdrawal |
| Structure activities that work at the client’s pace and activity. | Client can lose interest in activities that are too ambitious, which can increase a sense of failure. |
| Structure times each day to include planned times for brief interactions and activities with the client on one-on-one basis | Helps client to develop a sense of safety in a non-threatening environment. |
| If client is unable to respond verbally or in a coherent manner, spend frequent, short period with clients. | An interested presence can provide a sense of being worthwhile. |
| If client is found to be very paranoid, solitary or one-on-one activities that require concentration are appropriate. | Client is free to choose his level of interaction; however, the concentration can help minimize distressing paranoid thoughts or voice. |
| If client is delusional/hallucinating or is having trouble concentrating at this time, provide very simple concrete activities with client (e.g., looking at a picture or do a painting). | Even simple activities help draw client away from delusional thinking into reality in the environment. |
| If client is very withdrawn, one-on-one activities with a “safe” person initially should be planned. | Learn to feel safe with one person, then gradually might participate in a structured group activity. |
| Try to incorporate the strengths and interests the client had when not as impaired into the activities planned. | Increase likelihood of client’s participation and enjoyment. |
| Teach client to remove himself briefly when feeling agitated and work on some anxiety relief exercise (e.g., meditations,rhytmic exercise, deep breathing exercise). | Teach client skills in dealing with anxiety and increasing a sense of control. |
| Useful coping skills that client will need include conversational and assertiveness skills. | These are fundamental skills for dealing with the world, which everyone uses daily with more or less skill. |
| Remember to give acknowledgment and recognition for positive steps client takes in increasing social skills and appropriate interactions with others. | Recognition and appreciation go a long way to sustaining and increasing a specific behavior. |
| Provide opportunities for the client to learn adaptive social skills in a non-threatening environment. Initial social skills training could include basic social behaviors (e.g., appropriate distance, maintain good eye contact, calm manner/behavior, moderate voice tone). | Social skills training helps client adapt and function at a higher level in society, and increases client’s quality of life. |
| As client progresses, provide the client with graded activities according to level of tolerance e.g., (1) simple games with one “safe” person; (2) slowly add a third person into “safe”. | Gradually the client learns to feel safe and competent with increased social demands. |
As client progresses, Coping Skills Training should be available to him/her (nurse, staff or others). Basically the process:
|
Increases client’s ability to derive social support and decrease loneliness. Clients will not give up substance of abuse unless they have alternative means to facilitate socialization they belong. |
| Eventually engage other clients and significant others in social interactions and activities with the client (card games, ping pong, sing-a-songs, group sharing activities) at client’s level. | Client continues to feel safe and competent in a graduated hierarchy of interactions. |
