Notes
Definition
A sensory system is a part of the nervous system responsible for processing sensory information. A sensory system consists of sensory receptors, neural pathways, and parts of the brain involved in sensory perception. Commonly recognized sensory systems are those for vision, hearing, somatic sensation (touch), taste and olfaction (smell). In short, senses are transducers from the physical world to the realm of the mind.
Olfactory (Smell)
The nose has two primary functions. The first is olfaction – the sense of smell. However, the second function is of primary interest to this discussion – filtration, heating and humidification of the inhaled air. To accomplish the second task, the nasal cavity contains a convoluted set of passageways called the turbinates on the lateral wall of each nasal cavity.
The nose performs other various functions such as:
- Respiration.
- Air conditioning of the inspired air.
- Filtration of the inspired air.
- Olfaction or sense of smell.
- Resonating the spoken voice.
- Draining the para nasal sinuses and the nasolacrimal duct.
ANATOMY OF THE NOSE
The nose consists of the following:
- External nose – triangular-shaped projection in the center of the face.
- Nostrils – The two openings into the nasal passages.
- Nasal passages – passages that are lined with mucous membranes and tiny hairs (cilia) that help to filter the air and move nasal and sinus mucous to the back of the throat. Nasal passages are separated by the nasal septum.
- Septum – made up of cartilage and bone and covered by mucous membranes. The cartilage also gives support to the lower part of the nose and divides the nasal passages into right and left sides.
- Sinuses – four-paired, air-filled cavities.
OLFACTORY RECEPTORS AND THE SENSE OF SMELL
Chemoreceptors are those that respond to chemicals in solution for taste and olfaction. The olfactory receptors are believed to be sensitive to a much wider range of chemicals. Thousands of olfactory receptors occupy a postage stamp-sized area in the roof of each nasal cavity. These are the receptors for the sense of smell.
Air entering the nasal cavities must make a hairpin turn to enter the respiratory passageway below which causes more air to flow superiorly across the olfactory receptors, thus, intensifying the sense of smell. Olfactory receptor cells are special neurons that are equipped with olfactory hairs. Olfactory hairs are long cilia that protrude from the nasal epithelium and are continually bathed by a layer of mucus secreted by underlying glands.
When the receptors are stimulated by chemicals that are dissolved in the mucus, they transmit impulses along the olfactory filaments, which collectively make up the olfactory nerve (cranial nerve I) to the olfactory complex of the brain. It is in the brain that the interpretation of the odor occurs. The olfactory pathways are closely tied into the limbic system, the emotional-visceral part of the brain. Hence, olfactory impressions are long lasting and are very much part of our memories and emotions.
The olfactory receptors are extremely sensitive. Only a few molecules are required to activate them. Olfactory neurons tend to adapt rather quickly when they are exposed to unchanging stimulus of odor. This is the main reason why a woman stops smelling her own perfume but quickly picks up the scent of another person’s perfume.
Gustatory (taste)
TASTE BUDS AND SENSE OF TASTE
The tongue is a versatile organ with specialized functions like taste and speech. Beneath a cover of taste buds, the tongue is almost entirely made up of muscle. The muscles of the tongue are essential for its bodily movement and intrinsic manipulations, required for actions like speech, articulation, deglutition or swallowing, whistling, licking, kissing and even cleaning teeth.
Taste is the brain’s interpretation of chemicals that trigger receptors on the tongue, which are housed in the taste buds. The basic chemical components, are found in foods, toxins, and other ingested matter. Unappealing tastes are usually associated with toxins, as this is a defense mechanism preventing consumption. The chemicals bind their particular receptors and initiate signaling that travels through the nerves to the brain, where they are interpreted.
Taste Buds
The taste buds are specific receptors for the sense of taste which are widely distributed in the oral cavity. Of the 10,000 taste buds that humans have, most are located in the tongue. Few are found on the soft palate and inner surface of the cheeks.
Papillae – small peg-like projections that covers the dorsal surface of the tongue. These peg-like projections are of three types namely:
- Sharp filiform papillae
- Rounded fungiform papillae
- Circumvallate papillae
Taste buds are found on the sides of the circumvallate papillae but are more numerous on the fungiform papillae. When a person eats something, the specific cells that respond to the chemical dissolved in the saliva are epithelial cells called gustatory cells. Gustatory cells are surrounded by supporting cells in the taste bud. Their long microvilli, the gustatory hairs, protrude through the taste pore and when they are stimulated, they depolarize and impulses are transmitted to the brain. To carry the taste impulses three cranial nerves transports it to the gustatory cortex namely:
- Cranial nerve VII
- Cranial nerve IX
- Cranial nerve X
Auditory (hearing)
Overview
Hearing is one of the major senses and like vision is important for distant warning and communication. It can be used to alert, to communicate pleasure and fear. It is a conscious appreciation of vibration perceived as sound. In order to do this, the appropriate signal must reach the higher parts of the brain.
Functions of the ear
The ears are paired sensory organs comprising the auditory system, involved in the detection of sound, and the vestibular system, involved with maintaining body balance or the equilibrium. The ear divides anatomically and functionally into three regions: the external ear, the middle ear, and the inner ear. All three regions are involved in hearing. Only the inner ear functions in the vestibular system.
- SOUND DETECTION. The function of the ear is to convert physical vibration into an encoded nervous impulse. It can be thought of as a biological microphone. Like a microphone the ear is stimulated by vibration: in the microphone the vibration is transduced into an electrical signal, in the ear into a nervous impulse which in turn is then processed by the central auditory pathways of the brain.
- MAINTAINING BODY BALANCE or EQUILIBRIUM. The prime function of the vestibular system is to detect and compensate for movement. This includes the ability to maintain optic fixation despite movement and to initiate muscle reflexes to maintain balance.
Anatomy of the Ear
The ear is divided into three major areas: the outer or external ear, the middle ear and the inner or internal ear. The outer and middle ear are involved with hearing only whilst the inner ear functions both equilibrium and hearing.
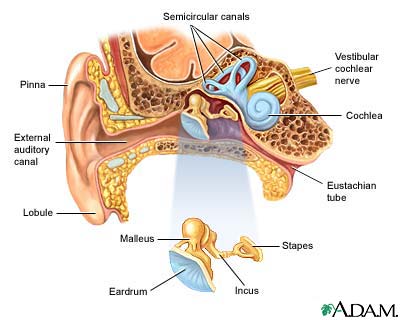
OUTER (EXTERNAL) EAR
The outer ear collects sound waves in the air and channels them to the inner parts of the ear. The outer ear along with its canal has been shown to enhance sounds within a certain frequency range. That range just happens to be the same range that most of the characteristics of human speech sounds fall into. This allows the sounds to be boosted to twice their original intensity. Parts of the outer ear are the following:
- Pinna – Also called the auricle. It is the part which protrudes from the side of the skull made of cartilage covered by skin. The pinna collects sound and channels it into the ear canal. The pinna’s shape enables it to funnel sound waves into the external auditory meatus. The various folds in the pinna’s structure amplify some high frequency components of the sound. They also help in the localization of sound in the vertical plane. As sounds hit the pinna from above and below, their paths to the external auditory meatus vary in length. This means that they take different times to reach the meatus.
- External acoustic meatus or external auditory canal – this is a short chamber about 1 inch long by ¼ inch wide. It is carved into the temporal bone of the skull. The canal has bends in both the vertical and horizontal planes. This means that it is difficult for anything poked into the meatus to hit the drum. Any trauma is likely to be to the walls of the canal. In its skin-lined walls are theceruminous glands, which secrete a waxy yellow substance, called earwax or cerumen.
Sound waves entering the external auditory canal eventually hit the tympanic membrane or eardrum and cause it to vibrate. The canal ends at the eardrum, which separates the outer ear from the middle ear.
MIDDLE EAR
The middle ear or tympanic cavity is an air filled space within the temporal bone. It transforms the acoustical vibration of the sound wave into mechanical vibration and passes it onto the inner ear. The three tiny bones of the middle ear act as a lever to bridge the eardrum with the oval window. Incoming forces are magnified by about 30 %. This increased force allows the fluid in the cochlea of the inner ear to be activated.
The tympanic cavity is spanned by the three smallest bones in the body, the ossicles which transmit the vibratory motion of the eardrum to the fluids of the inner ear. These bones, named for their shape, are the following:
- Hammer or malleus
- Anvil or incus
- Stirrup or stapes
When the eardrum moves the hammer moves with it and transfers the vibration to the anvil. In response to this, the anvil passes it on to the stirrup which in turn presses on the oval window of the inner ear. The movement of the oval window sets the fluids of the inner ear into motion, eventually exciting the hearing receptors.
The Eustachian tube is a canal that links the middle ear with the throat area. This tube helps to equalize the pressure between the outer ear and the middle ear. Having the same pressure allows for the proper transfer of sound waves. The eustachian tube is lined with mucous, just like the inside of the nose and throat.
INNER EAR
The inner ear consists of a maze of fluid-filled tubules running through the temporal bone of the skull. The bony tubes, the bony labyrinth, are filled with a fluid called perilymph. Within this bony labyrinth is a second series of delicate cellular tubes, called the membranous labyrinth, filled with the fluid called endolymph. This membranous labyrinth contains the actual hearing cells, the hair cells of the organ of Corti.
There are three major sections of the bony labyrinth:
- The front portion is the snail-shaped cochlea, which functions in hearing
- The rear part, the semicircular canals, helps maintain balance
- Interconnecting the cochlea and the semicircular canals is the vestibule, containing the sense organs responsible for balance, the utricle and saccule.
The bony cochlea is so called because it is shaped like a snail shell It has two and a half turns and houses the organ of hearing known as the membranous labyrinth surrounded by fluid called the perilymph. The cochlea has a volume of about 0.2 of a millilitre. In this space lie up to 30,000 hair cells which transduce vibration into nervous impulses and about 19,000 nerve fibers which transmit the signals to and from the brain.
The inner ear has two membrane-covered outlets into the air-filled middle ear – the oval window and the round window. The oval window sits immediately behind the stapes, the third middle ear bone, and begins vibrating when “struck” by the stapes. This sets the fluid of the inner ear sloshing back and forth. The round window serves as a pressure valve, bulging outward as fluid pressure rises in the inner ear. Nerve impulses generated in the inner ear travel along the vestibulocochlear area (cranial nerve VIII), which leads to the brain. This is actually two nerves, somewhat joined together, the cochlear nerve for hearing and the vestibular nerve for equilibrium.
How Do We Hear?
The range of audible sound is approximately 10 octaves from somewhere between 16 and 32 Hz (cycles per second) to somewhere between 16,000 and 20,000 Hz. The sensitivity is low at the extremes but becomes much more sensitive above 128 Hz up to about 4,000 Hz when it again becomes rapidly less sensitive. The range of maximum sensitivity and audibility diminishes with age.
What Do We Hear?
All sounds (music, voice, a mouse-click, etc.) send out vibrations, or sound waves. Sound waves do not travel in a vacuum, but rather require a medium for sound transmission, e.g. air or fluid. What actually travels are alternating successions of increased pressure in the medium, followed by decreased pressure.
Hearing starts with the outer ear. When a sound is made outside the outer ear, the sound waves, or vibrations, travel down the external auditory canal and strike the eardrum (tympanic membrane). The eardrum vibrates. The vibrations are then passed to three tiny bones in the middle ear called the ossicles. The ossicles amplify the sound and send the sound waves to the inner ear and into the fluid-filled hearing organ (cochlea).
Once the sound waves reach the inner ear, they are converted into electrical impulses which the auditory nerve sends to the brain. The brain then translates these electrical impulses as sound.
The mechanism of hearing is summarized below:
- Sound
- Pinna collects the sound heard
- External auditory canal
- Vibration in the ear drum is produced
- Amplified by the ossicular chain. The sound is then transmitted to the inner ear.
- The cochlea converts the sound vibration to electrical impulses. Within the cochlear duct, the endolymph-containing membranous labyrinth of the snail-like cochlea is the organ of Corti, which contains the hearing receptors or hair cells. The chambers above and below the cochlear duct contain perilymph. Sound waves that reach the cochlea through vibrations of the eardrum, ossiscles and oval window set cochlear fluids into motion.
- The hair cells transmit impulses along the cochlear nerve or auditory nerve (a division of cranial nerve VIII – the vestibulocochlear nerve) to the auditory cortex in the temporal lobe.
- Auditory cortex interprets the sound, or hearing occurs.
Since sound usually reaches the two ears at different times, a person can hear “in stereo,” which functionally helps humans differentiate where sounds are coming from the environment. In cases where the sounds or tones keep reaching the ears, the auditory receptors tend to adapt or stop responding to these sounds, thus the person becomes no longer aware of them. Important information about hearing is the fact that it is the last sense to leave the awareness when a person falls asleep or receives anesthesia or dies. As a person awakens from sleep, it is the first sense to return.
Vision (sight)
Overview
A person’s sense of sight is very important to humans. Vision is arguably the most used of the 5 senses and is one of the primary means that we use to gather information from our surroundings. The human eye is the organ which gives us the sense of sight, allowing us to observe and learn more about the surrounding world than we do with any of the other four senses.
People use their eyes in almost every activity they perform, whether reading, working, watching television, writing a letter, driving a car, and in countless other ways. Most people probably would agree that sight is the sense they value more than all the rest. The eyes are at work from the moment a person is wake up to the moment he or she closes them to go to sleep.
This special organ takes in tons of information about the world around you — shapes, colors, movements, and more. Then they send the information to your brain for processing so the brain knows what’s going on outside of your body.
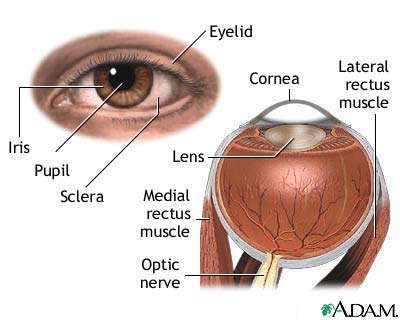
Anatomy of the Eye
External and Accessory Structures
The adult eye is a sphere-shaped organ that measures about 1 inch or 2.5 cm in diameter. However, only one sixth (1/6) of the eye’s surface can normally be seen and the rest is enclosed and protected by a cushion of fat and the walls of the bony orbit.
The accessory structures of the eye are the following:
- Extrinsic eye muscles. The extrinsic muscles of the eye come from the bones of the orbit and are movable due to broad tendons in the eye’s tough outer surface. There are six extrinsic eye muscles that function to MOVE the eye in various directions:
- Superior rectus muscle – rotates the eye upward and toward the midline
- Inferior rectus muscle – rotates the eye downward and toward the midline
- Medial rectus – rotates the eye toward the midline
- Lateral rectus – rotates the eye away from the midline
- Superior oblique – rotates the eye downward and away from the midline
- Inferior oblique – rotates the eye upward and away from the midline
- Eyelids. The eyelids protect the eyes anteriorly which meet at the medial and the lateral corners of the eye. From the border of each eyelid are the EYELASHES. The eyelashes help filter out foreign matter, including dust and debris, and prevent it from getting into the eye. Eyelid edges associate with modified sebaceous glands make up the TARSAL GLANDs. These glands produce an oily secretion that lubricates the eye. Between the eyelashes, modified sweat glands called ciliary glands are found.
- Conjunctiva. The conjunctiva is a mucous membrane that begins at the edge of the cornea and lines the inside surface of the eyelids and sclera, which serves to lubricate the eye. It is the thin, transparent tissue that covers the outer surface of the eye. This structure is nourished by tiny blood vessels that are nearly invisible to the naked eye. The conjunctiva is composed of 3 sections:
- Palpebral Conjuctiva – covers the posterior surface of the eyelids
- Bulbar Conjuctiva – coats the anterior portion of the eyeball
- Fornix – the transition portion, forming the junction between the posterior eyelid and the eyeball
NOTE: Although the palpebral conjunctiva is moderately thick, the bulbar conjunctiva is very thin. The latter also is very movable, easily sliding back and forth over the front of the eyeball it covers. Since it is clear, blood vessels are easily visible underneath it.
Within the bulbar conjunctiva are “goblet cells,” which secrete “mucin.” This is an important component of the pre-corneal tear layer that protects and nourishes the cornea.
- Lacrimal Apparatus. The lacrimal apparatus consists of the lacrimal gland and a number of ducts that drain the lacrimal secretions into the nasal cavity. Located above the lateral end of each eye are the lacrimal glabds that continually release a dilute salt solution, known as tears, onto the anterior surface of the eyeball through several small ducts. The flow of tears flush across the following structures orderly:
- Eyeball
- Lacrimal canals medially
- Lacrimal sac
- Nasolacrimal duct that empties into the nasal cavity.
Lacrimal secretion contains antibodies and an enzyme that destroys bacteria known as lysozyme. Hence, tears cleanse and protect the eye surface as it moistens and lubricates it. in cases when lacrimal secretion substantially increases, tears spill over the eyelids and fill the nasal cavities. This causes congestion and the “sniffles.” When eyes are irritated by foreign objects or chemicals and when a person is emotionally upset lacrimal secretion is stimulated and increased.
Internal Eye structures
The Eyeball
The eye, commonly called the eyeball, is a hollow sphere and is composed of:
- 3 tunics or coats
- Humors – the interior filled with fluids that help maintain the shape of the eye
- Lens – the main focusing apparatus of the eye. This structure is supported within the eye cavity dividing it into two chambers.
TUNICS of the EYEBALL
- Fibrous Tunic – this is the outermost tunic and is also known as the sclera, the thick and white connective tissue. The fibrous tunic (sclera) is seen anteriorly as the “white part of the eye.” The central portion of this tunic is modified so that it is crystal clear. The cornea is the transparent “window” through which light enters the eye and is well supplied with nerve endings. This is the main reason why blinking and increased tearing occur when the cornea is touched because most nerve endings found here are pain fibers.
- Vascular tunic – this is the middle coat of the eyeball and has three distinguishable regions namely:
- Choroid – this is located posteriorly and lies between the sclera and the retina. It contains the blood vessels that provide nourishment to the outer layers of the retina. It is composed of layers of blood vessels that nourish the back of the eye. The choroid is opaque and deeply pigmented with melanin to absorb excessive light; else internal reflection would form multiple images on the retina. It is less vascular where the retina is thin. The choroid connects with the ciliary body toward the front of the eye and is attached to edges of the optic nerve at the back of the eye.
2. Ciliary Body – the ciliary body is made up of ciliary muscles and ciliary processes. It lies just behind the iris. This is the structure to which lens are attached by a suspensory ligament called the ciliary zonule and then the iris. The pigmented iris has a rounded opening, the pupil, through which light passes. Nourishment for the ciliary body comes from blood vessels which also supply the iris. Ciliary processes are short, black tissues arranged radially. They secrete aqueous humour.
One function of the ciliary body is the production of aqueous, the clear fluid that fills the front of the eye. It also controls accommodation by changing the shape of the crystalline lens. When the ciliary body contracts, the zonules relax. This allows the lens to thicken, increasing the eye’s ability to focus up close. When looking at a distant object, the ciliary body relaxes, causing the zonules to contract.
3. Sensory Tunic – this is the innermost tunic of the eye and is called the retina. This structure extends anteriorly only to the ciliary body. It converts images into electrical impulses that are sent along the optic nerve to the brain where the images are interpreted. The retina can be compared to the film of a camera. It contains millions of receptor cells, the rods and cones. Rods and cones are called photoreceptors because they respond to light.
The rods and cones are not distributed evenly in the retina. The rods are most dense at the periphery or edge of the retina and decrease in number as the center of the retina is approached. It is more numerous, some 120 million, and are more sensitive than the cones. However, they are not sensitive to color. The 6 to 7 million cones provide the eye’s color sensitivity and they are much more concentrated in the central yellow spot known as the macula. In the center of that region is the fovea centralis a 0.3 mm diameter rod-free area with very thin, densely packed cones. Consequently, this is the area of greatest visual acuity or the point of sharpest vision and anything we wish to view critically is focused on the fovea centralis.
The photoreceptor cells are distributed over the entire retina, except where the optic nerve leaves the eyeball. This is the site called the optic disc or blind spot. When light from an object is focused on the optic disc, it disappears from our point of view and we cannot see it.
LENS
The crystalline lens is located just behind the iris. Light entering the eye is focused on the retina by the lens. The nucleus, the innermost part of the lens, is surrounded by softer material called the cortex. The lens is encased in a capsular-like bag. It is held upright in the eye by a suspensory ligament, the ciliary zonule, attached to the ciliary body. Together, the lens and the ciliary body help control fine focusing of light as it passes through the eye. The lens is divided into two segments namely:
- Anterior (aqueous) segment – located anterior to the lens and contains a clear wayetry fluid called aqueous humor. The aqueous humor helps to nourish the cornea and the lens. It is continually produced by the ciliary body.
- Posterior (vitreous) segment – located posterior to the lens and is filled with a gel-like substance called the vitreous humor or the vitreous body. The vitreous is a thick, transparent substance that fills the center of the eye. It is composed mainly of water and comprises about 2/3 of the eye’s volume, giving it form and shape. The viscous properties of the vitreous allow the eye to return to its normal shape if compressed. The vitreous humor helps maintain the shape of the eye.
image courtesy of health.allrefer.com, medical-dictionary.thefreedictionary.com, walgreens.com, genericlook.com, medicalook.com, health.howstuffworks.com,umm.edu


