Notes
Description
- Parkinson’s disease is a degenerative disease caused by depletion of dopamine, which interferes with the inhibition of excitatory impulses.
- Parkinson’s disease results in a dysfunction of the extrapyramidal system.
- Parkinson’s disease is a slow, progressive disease that results in a crippling disability.
- The debilitation can result in falls self-care deficits, failure of body systems, and depression.
- Mental deterioration occurs late in the disease.
Cause
The majority of all cases of classic Parkinson’s disease are primary, or idiopathic, Parkinson’s disease (IPD). The cause is unknown; a few cases suggest a hereditary pattern. Secondary, or iatrogenic, Parkinson’s disease is drug- or chemical-related. Dopamine-depleting drugs such as reserpine, phenothiazine, metoclopramide, tetrabenazine, and the butyrophenones (droperidol and haloperidol) can lead to secondary Parkinson’s disease.
Assessment
- Bradykinesia, abnormal slowness of movement, and sluggishness of physical and mental responses.
- Akinesia
- Monotonous speech
- Handwriting that becomes progressively smaller
- Tremors in hands and fingers at rest (pill rolling)
- Tremors increasing when fatigued and decreasing with purposeful activity or sleep.
- Rigidity with jerky interrupted movements
- Restlessness and pacing
- Blank facial expression-mask –like facies
- Drooling
- Difficulty swallowing and speaking
- Loss of coordination and balance.
- Shuffling steps, stooped position, and propulsive gait.
Primary Nursing Diagnosis
- Self-care deficit related to rigidity and tremors
Diagnostic Evaluation
- The diagnosis of Parkinson’s disease is usually made through clinical findings rather than diagnostic tests. The key to diagnosis is the patient’s response to levodopa (see Pharmacologic Highlights).
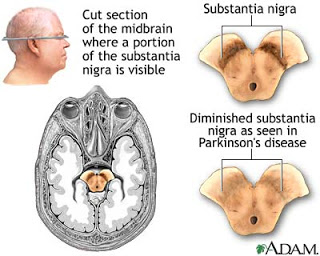
- Positron emission tomography (PET) and single photon emission computed tomography (SPECT) shows decrease dopamine uptake in the basal ganglia. Degeneration of substantia nigra in the basal ganglia of midbrain leads to depletion of dopamine
Medical Management
- To control tremor and rigidity, pharmacologic management is the treatment of choice. Longterm levodopa therapy can result in drug tolerance or drug toxicity. Symptoms of drug toxicity are confusion, hallucinations, and decreased drug effectiveness. Treatment for drug tolerance and toxicity is either a change in drug dosage or a drug holiday.
- Autologous transplantation of small portions of the adrenal gland into the brain’s caudate nucleus of Parkinson’s disease patients is offered on an experimental basis in some medical centers as a palliative treatment. In addition, if medications are ineffective, a thalamotomy or stereotaxic neurosurgery may be done to treat intractable tremor.
- Physical and occupational therapy consultation is helpful to plan a program to reduce flexion contractures and to maximize functions for the activities of daily living. To prevent impaired physical mobility, perform passive and active range-of-motion exercises and muscle-stretching exercises. In addition, include exercises for muscles of the face and tongue to facilitate speech and swallowing. Use of a cane or walker promotes ambulation and prevents falls.
Pharmacologic Highlights
- Antiparkinson drugs such as Levodopa (L-dopa); carbidopa-levodopa (Sinemet) is used to control tremors and rigidity; converted to dopamine in the basal ganglia.
- Antiviral agents such as Amantadine hydrochloride (Symmetrel) is used to control tremor and rigidity by increasing the release of dopamine to the basal ganglia.
- Synthetic anticholinergics such as Trihexyphenidyl (Artane); benztropine mesylate (Cogentin) is used to block acetylcholine stimulated nerves that lead to tremors.
- Other Drugs: Antihistamines are sometimes prescribed with the anticholinergics to inhibit dopamine uptake; bromocriptine mesylate, a dopamine antagonist, is ordered to stimulate dopaminergic receptors.
Nursing Interventions
- Assess neurological status.
- Assess ability to swallow and chew.
- Provide high-calorie, high-protien, high-fiber soft diet with small, frequent feedings.
- Increase fluid intake to 2000 mL/day.
- Monitor for constipation.
- Promote independence along with safety measures.
- Avoid rushing the client with activities.
- Assist with ambulation and provide assistive devices.
- Instruct client to rock back and forth to initiate movement.
- Instruct the client to wear low-heeled shoes.
- Encourage the client to lift feet when walking and avoid prolonged sitting.
- Provide a firm mattress, and position the client prone, without a pillow, to facilitate proper posture.
- Instruct in proper posture by teaching the client to hold the hands behind the back to keep the spine and neck erect.
- Promote physical therapy and rehabilitation.
- Administer anticholinergic medications as prescribed to treat tremors and rigidity and to inhibit the action of acetylcholine.
- Administer antiparkinsonian medications to increase the level of dopamine in the CNS.
- Instruct the client to avoid foods high in vitamin B6 because they block the effects of antiparkinsonian medications.
- Instruct the client to avoid monoamine oxidase inhibitors because they will precipitate hypertensive crisis.
Documentation Guidelines
- Ability to ambulate, perform the activities of daily living, progress in an exercise program
- Use of verbal and nonverbal communication
- Statements about body image and self-esteem
- Discomfort during activity
Discharge and Home Healthcare Guidelines
- Be sure the patient or caregiver understands all medications, including the dosage, route, action, and adverse reactions. Avoid the use of alcohol, reserpine, pyridoxine, and phenothiazine while taking levodopa.
- In general, recommend massage and relaxation techniques, and reinforce exercises recommended by the physical therapist. Several techniques facilitate mobility and enhance safety in Parkinson’s disease patients. Instruct the patient to try the following strategies:
- To assist in maintaining balance, concentrate on taking larger steps with feet apart, keeping back straight and swinging the arms;
- To overcome akinesia, tape the “frozen” leg to initiate movement;
- To reduce tremors, hold objects (coins, keys, or purse) in the hand;
- To obtain partial control of tremors when seated, grasp chair arms;
- To reduce rigidity before exercise, take a warm bath;
- To initiate movement, rock back and forth;
- To prevent spine flexion, periodically lie prone and avoid using a neck pillow; and
- Teach the patient to eliminate loose carpeting, install grab bars, and elevate the toilet seat. Use of chair lifts can also be beneficial.
Exam
Nursing Care Plan
Nursing Diagnosis
Ineffective Airway Clearance
May be related to
- parkinsonian changes in musculature
- tracheobronchial obstruction
- aspiration
- infection
- truncal rigidity
- bronchospasm
- fatigue
- increased work of breathing
- increased mucus production
- thick secretions
Possibly evidenced by
- dyspnea
- tachypnea
- bradypnea
- bronchospasms
- increased breathing effort
- use of accessory muscles
- increased mucus production
- cough with or without productivity
- adventitious breath sounds
- abnormal arterial blood gases
Desired Outcomes
- Patient will achieve the normalization and ability to maintain patent airways and respiratory status.
- Patient will achieve and maintain patent airway.
- Patient will have clear breath sounds to auscultation, and will have respiratory status parameters with optimal air exchange.
- Patient will be able to cough up secretions and perform coughing and deep breathing exercises.
Nursing Interventions
- Observe patient and assess energy level and endurance, and how these affect respiratory status.
- Rationale: Energy ability decreases with age and chronic disease like PD.
- Assess respiratory status for rate, depth, ease, use of accessory muscles, and work of breathing.
- Rationale: For baseline data.
- Auscultate the lung fields for presence of wheezes, crackles, rhonchi, or decreased breath sounds.
- Rationale: Wheezing results from squeezing of air past the narrowed airways during expiration which is caused by bronchospasms, edema, and obstructive secretions. Crackles result from consolidation of leukocytes and fibrin in the lung causing an infection or by fluid accumulation in the lungs. Decreased breath sounds may indicate alveolar collapse with little to no air exchange in the lung area being auscultated, and usually results in poor ventilation.
- Administer oxygen as ordered. Monitor oxygen saturation by pulse oximetry.
- Rationale: Provide supplemental oxygen to benefit patient.
- Assess patient for pallor or cyanosis in nail beds and/or around the mouth.
- Rationale: May indicate hypoxemia.
- Monitor patient for cough and production of sputum, noting amount, color, character, and patient’s ability to expectorate secretions and patient’s ability to cough.
- Rationale: Mucus color from yellow to green may indicate presence of infection. Tenacious, thick secretions require more effort and energy to cough up and remove, and may cause obstruction and stasis that may lead to infection.
- Position patient in high Fowler’s or semi-Fowler’s position, if possible.
- Rationale: Promotes maximal lung expansion.
- Turn patient every 2 hours.
- Rationale: Repositioning promotes drainage of pulmonary secretions and enhances ventilation to decrease potential for atelectasis.
- Administer bronchodilators as ordered.
- Rationale: Promotes relaxation of bronchial smooth muscles to decrease spasm, dilates airways to improve ventilation, and maximizes air exchange.
- Encourage increase in intake of fluids up to 3-4 L/day.
- Rationale: Provides hydration and helps to thin secretions for easier mobilization and removal.
- Perform postural drainage and percussion as ordered.
- Rationale: Postural drainage utilizes gravity to help raise secretions and clear sputum. Percussion may assist in movement of secretions away from bronchial walls and enable patient to cough them up and increase the force of expiration. Some positions done may be contraindicated in elderly patients.
- Encourage deep breathing and coughing exercises every 2 hours.
- Rationale: Assist in lung expansion and helps in dislodgement of secretions for easier expectoration.
- Suction patient if warranted.
- Rationale: Patient may be too weak or fatigued to expel own secretions.
- Instruct patient to seek help and stop smoking of patient is a smoker.
- Rationale: Smoking causes increased mucus, vasoconstriction, and increased blood pressure.
Nursing Diagnosis
Disturbed Thought Process
May be related to
- parkinsonian medications
- psychological causes
- depression
- incorrect belief system
- chronic illness
- misperceptions
Possibly evidenced by
- inaccurate interpretation of environment
- changes in lifestyle
- loss of significant other
- egocentricity
- distractibility
- inappropriate thinking
- memory impairment
- sorrow
- hypovigilance or hypervigilance
- chronic illness
- insomnia
- inability to perform activities as before
- abnormal lab studies
- uncaring attitude
- toxic levels of medications
- akinesia
Desired Outcomes
- Patient will identify factors that elicit depressive reactions and use techniques that will effectively reduce the amount and frequency of these episodes.
- Patient will be compliant with the therapeutic regimen.
Nursing Interventions
- Assess patient for depressive behaviors, causative events, and orient patient to reality as warranted.
- Rationale: Depression is a common among PD patients, whether it’s a reaction to the disorder or related to biochemical abnormality is uncertain. Identify specific problems and allow for the establishment of a plan of care. Reality orientation helps patient to be aware of self and surroundings.
- Use nonjudgmental attitude toward patient and actively listen to his feelings and concerns.
- Rationale: Establishes a trusting relationship and permits patient to discuss topics that can help the patient deal with in appropriate ways. PD patients often feel embarrassed apathetic, bored, and lonely that may be brought about by physical slowness and the great effort that even small tasks require. Encourage and assist the patient in every effort possible to carry out the tasks involved in meeting their own daily needs to remain independent.
- Identify patient’s medications currently being taken.
- Rationale: Assists with identification of any misuse of drugs and side-effects that may precipitate depressive symptoms.
- Assess patient for potential for suicide and suicidal ideation.
- Rationale: Patients who are depressed and who have already thought about a suicide plan are serious and need emergency help.
- Monitor vital signs every 4 hours and prn.
- Rationale: Antidepressants and other psychoactive medications may result in cardiovascular and cerebrovascular insufficiency. Amantadine(Symmetrel) can cause psychiatric disturbances, mood changes, hallucinations.
Nursing Diagnosis
Impaired Verbal Communication
May be related to
- physical barrier from hypertonicity from parkinsonism
- rigidity of facial muscles
- depression medications
- psychological barriers
- psychosis
- depression
- medications
- psychological barriers
- psychosis
- decreased circulation to brain
- age-related factors
- lack of stimuli
Possibly evidenced by
- confusion, anxiety, restlessness
- flight of ideas
- inability to speak
- stuttering
- impaired articulation
- difficulty with phonation
- inability to name words
- inability to identify objects
- difficulty comprehending communication
- dyslalia
- dysarthria
- inappropriate verbalizations
- aphasia
- dysphasia
- apraxia
- slurred
- slow monotonous speech
- high-pitched rapid speech, repetitive speech
- facial muscle rigidity
Desired Outcomes
- Patient will be able to have effective speech and understanding of communication, or will be able to use another method of communication and make needs known.
- Patient will be able to use assistive devices and techniques to improve ability to communicate.
- Patient will be able to speak in an understandable way possible when necessary.
- Patient will be able to understand communication.
- Patient will be able to exhibit minimal frustration and anxiety with speech attempts.
- Patient will be able to make needs known utilizing nonverbal methods if required.
- Family will be compliant and supportive of patient’s attempt at communication.
Nursing Interventions
- Assess the patient’s ability to speak, language deficit, cognitive or sensory impairment, presence of aphasia, dysarthria, aphonia, dyslalia, or apraxia. Presence of psychosis, and/or other neurologic disorders affecting speech.
- Rationale: Speech disorders are present in most patients with Parkinson’s disease, this helps identify problem areas and speech patterns to help establish a plan of care.
- Instruct patient to make a conscious effort to speak slowly, with deliberate attention to what they’re speaking. Remind the patient to face the listener, exaggerate the pronunciation of words, speak in short sentences, and take a few breaths before speaking.
- Rationale: This helps establish a clear method of communication and speaking to the patient.
- Monitor the patient for nonverbal communication, such as facial grimacing, smiling, pointing, crying, and so forth; encourage use of speech when possible.
- Rationale: Indicates that feelings or needs are being expressed when speech is impaired. Excessive mumbling, striking out, or non verbalization clues may b e the only method left for the patient to express discomfort.
- Attempt to anticipate patient’s needs.
- Rationale: Helps to prevent frustration and anxiety.
- When communicating with patient, face patient and maintain eye contact, speaking slowly and enunciating clearly in a moderate or low-pitched tone.
- Rationale: Clarity, brevity, and time provided for responses promotes the opportunity for successful speech by allowing patient time to receive and process the information.
- Remove competing stimuli, and provide a calm, unhurried atmosphere for communication.
- Rationale: Reduces unnecessary noise and distraction and allows patient time to decrease frustration.
- Use simple, direct questions requiring one-word answers. Repeat and reword questions if misunderstanding occurs.
- Rationale: Promotes self-confidence of the patient who is able to achieve some degree of speech or communication.
- Provide a small electronic amplifier if necessary.
- Rationale: Helpful if the patient has difficulty being heard.
- Encourage patient to control the length and rate of phrases, over articulate words, and separate syllables, emphasizing consonants.
- Rationale: Helps to promote speech in the presence of dysarthria.
- Avoid rushing the patient when struggling to express feelings and thoughts.
- Rationale: Impaired verbal communication results in patient’s feeling of isolation, despair, depression, and frustration. Compassion helps to foster a therapeutic relationship and sense of trust and is important for continuing communication.
- Instruct patient and/or SO regarding need to use glasses, hearing aids, dentures.
- Rationale: Helps promote communication with sensory or other deficits.
- Instruct patient and/or SO in the performance of facial muscle exercises, such as smiling, frowning, sticking tongue out, moving tongue from side to side and up and down.
- Rationale: Promotes facial expressions used to communicate by increasing muscle coordination and tone.
Nursing Diagnosis
Impaired Physical Mobility
May be related to
- Parkinson’s disease
- dementia
- inability to bear weight
- poor nutrition
- perceptual impairment
- cognitive impairment
- tremors
- rigidity
- bradykinesia
Possibly evidenced by
- Inability to move at will
- weakness
- inability to bear weight
- immobility
- gait disturbances
- balance and coordination deficits
- difficulty turning
- decreased fine and gross motor movement
- decreased reaction time
- incoordination
- jerky movement
- swaying
- postural disturbances
- small, shuffling gait
Desired Outcomes
- Patient will maintain functional mobility as long as possible within limitations of disease process.
- Patient will have few, if any, complications related to immobility.
Nursing Interventions
- Instruct patient with techniques that initiate movement.
- Rationale: Rocking from side to side helps to start the leg movement.
- Instruct patient to get out of chair by moving to edge of seat, placing hands on arm supports, bending forward, and then rocking to a standing position.
- Rationale: Parkinson disease causes rigidity tremors, bradykinesia and may result in difficulty getting out of a chair.
- Teach the patient to concentrate on walking erect and use a wide-based gait.
- Rationale: Balance may be adversely affected because of the rigidity of the arms that prevents them from swinging when walking normally. A special walking technique must be learned to offset the shuffling gait and the tendency to lean forward. A conscious effort must be made to swing the arms, raise the feet while walking, and use a heel-toe placement of the feet with long strides.
- Instruct patient to perform daily exercise that will increase muscle strength: walking, riding a stationary bike, swimming, and gardening are helpful.
- Rationale: Exercise prevents contractures that occur when muscles are not used, improves coordination and dexterity, and reduces muscular rigidity. Adherence to exercise and walking program helps delay the progress of the disease.
- Teach patient to sit in chairs with backs and arm rests; use elevated toilet seats or sidebars in the bathroom.
- Rationale: Help with rising from a sitting position and prevent falls.
- Recommend that seuxal relations be planned for when the medication is active.
- Rationale: Parkinson’s causes bradykinesia which can impair intimacy.
- Instruct patient to raise head of bed and make position changes slowly. Teach patient to dangle legs a few minutes before standing. Avoid dehydration and maintain adequate dietary salt.
- Rationale: These measures reduce orthostatic hypotension.
- Refer patient to a physical therapist.
- Rationale: May be helpful in developing an individualized exercise program and can provide instruction to the patient and caregiver on exercising safely.
- Provide warm baths and massages.
- Rationale: Helps relax muscles and relieve painful muscle spasms that accompany rigidity.
Nursing Diagnosis
Imbalanced Nutrition: Less Than Body Requirements
May be related to
- parkinsonian changes in musculature
- facial rigidity
- use of antiparkinsonian drugs
- inability to take in enough food
- decreased level of consciousness
- inability to absorb nutrients because of biologic or psychological factors from aging process
Possibly evidenced by
- inadequate food intake
- weight loss
- absent bowel sounds
- decreased peristalsis
- muscle mass loss
- decreased muscle tone
- changes in bowel habits
- nausea
- abdominal distention
- lack of interest in food
- fatigue from work of breathing
- choking, coughing
- rigidity of facial muscles
Desired Outcomes
- Patient will have adequate nutritional intake with no weight or muscle mass loss.
- Patient will maintain adequate nutritional status with use of nutritional support, and will experience no complications from support.
- Patient will show no signs of malnutrition status.
Nursing Interventions
- Assess patient’s ability to eat.
- Rationale: To provide information regarding factors associated with reduced intake of nutrients.
- Weigh patient daily, on the same scale and same time if possible.
- Rationale: Provides information about weight loss or gain.
- Provide an unhurried environment during meal time.
- Rationale: Patients with PD may have difficulty maintaining their weight as eating becomes a very slow process, requiring concentration due to a dry mouth from medications and difficulty chewing and swallowing.
- Monitor weight on a weekly basis.
- Rationale: To assess whether caloric indicate is adequate.
Nursing Diagnosis
Impaired Swallowing
May be related to
- Parkinson’s disease
- neuromuscular impairment
- dysphagia
Possibly evidenced by
- inability to swallow effectively
- choking
- aspiration
- food remaining in oral cavity
- slow eating
- difficulty swallowing
- chewing
- stiff
- masklike face
- choking, drooling
- weight loss
- facial rigidity
- muscle rigidity
- tremors
- aspiration
Desired Outcomes
- Patient will be able to swallow effectively with no incidence of aspiration.
- Patient will be able to eat and swallow normally.
- Patient will be able to ingest an adequate amount of nutrients without dangers of aspiration.
- Patient will be able to follow instructions and strengthen muscles used for eating and swallowing.
Nursing Interventions
- Evaluate patient’s ability to swallow, extent of paralysis, and ability to maintain airway.
- Rationale: Swallowing difficulties and choking are common in PD, evaluation provides baseline information from which to plan interventions for care.
- Maintain head position and support, with head of bed elevated at least 30 degrees or more during immediately after feeding.
- Rationale: Helps to prevent aspiration; facilitates ability to swallow.
- Instruct patient to chew sugarless chewing gum or suck on hard candy.
- Rationale: To keep his mouth moist and easy dryness of the mouth, a side effect of medications for PD.
- Place food in the unaffected side of patient’s mouth.
- Rationale: Allows for sensory stimulation and taste, and may assist to trigger swallowing reflexes.
- Provide foods that are soft and require little chewing; provide thickened liquids if possible. Avoid thin liquids.
- Rationale: These types of foods are easier to control and decrease potential for choking or aspiration.
- Administer tube feedings or enteral alimentation as warranted/ordered.
- Rationale: May be required if oral intake is not sufficient.
- Instruct patient and/or family to use straw for drinking liquids.
- Rationale: Helps strengthen facial oral muscles to decrease potential for choking.
- Teach patient to place food in tongue, close the lips and teeth, lift the tongue up and then back, and swallow. Encourage the patient to chew first on one side of the mouth and then on the other.
- Rationale: Proper technique to prevent aspiration.
- Instruct patient to make conscious effort to swallow.
- Rationale: To control the buildup of saliva.
- Massage the facial and neck muscles before meals.
- Rationale: Can help during meal time.
Nursing Diagnosis
Risk for Injury
May be related to
- Parkinson’s disease
- dementia
- lack of awareness of environmental hazards
- poor judgement
- medications
- hallucinations
- choking
- bradykinesia
- akinesia
Risk factors
- confusion
- disorientation
- malnutrition
- altered mobility
- skin breakdown
- agitation
- physical discomfort
- choking
- wounds
- falls
- wandering
- involuntary movements
- loss of postural adjustment
- loss of balance
- loss of arm swinging movement
- difficulty initiating movement
- shuffling gait
- slowness of movement
- orthostatic hypotension
- activity intolerance
- polypharmacy
- hallucinations
- tremors
- muscle rigidity
Desired Outcomes
- Patient will remain safe from environmental hazards resulting from cognitive impairment.
- Family will ensure safety precautions are instituted and followed.
- Patient will remain in a safe environment with no complications or injuries obtained.
- Family will be able to identify and eliminate hazards in the patient’s environment.
Nursing Interventions
- Assess ambulation and movement.
- Rationale: Aids in planning of interventions.
- Instruct patient to swing arms and lift heels during ambulation.
- Rationale: These action assist gait and prevent falls.
- Teach patient to turn in wide arcs.
- Rationale: To prevent the crossing of one leg over the other, which could cause a fall.
- Remind patient to maintain an upright posture and look up when walking.
- Rationale: Stooped posture may cause the patient to collide with objects.
- Instruct a wide-based gait
- Rationale: To improve balance.
- Teach range of motion exercises and stretching to be performed daily.
- Rationale: Exercising increases flexibility and improves strength and balance.
Nursing Diagnosis
Ineffective Coping
May be related to
- progressive chronic disease
- limitations imposed by disease
- depression
- lack of coping skills
- physical or emotional impairment caused by normal aging changes or parkinsonism
- changes in lifestyle
Possibly evidenced by
- verbalization of inability to cope
- inappropriate coping strategies
- social withdrawal
- irritability
- aggressiveness
- hostility
- changes in communication pattern
- inability to ask for help
- fatigue
- increased illness
- poor concentration
- decreased problem-solving skills
- risk-taking behaviors
- poor-self esteem
- insomnia
Desired Outcomes
- Patient will exhibit improvement in emotional well-being.
- Patient will use acceptable strategies to cope with problems, and will have improved sense of self-worth.
- Patient will be able to access support systems, community resources, or counselors to assist in achieving adequate coping skills.
Nursing Interventions
- Provide care for patient using same personnel whenever possible.
- Rationale: Provides for continuity of care and the establishment of a trusting relationship.
- Provide uninterrupted time to be spent with patient, and encourage him to express feelings and concerns.
- Rationale: Allows patient time to express extreme and powerful emotional feelings, and with discussion, patient can begin to comprehend the personal meaning attached to recent events and develop a reasonable assessment of the situation in order to identify a plan to deal constructively with the situation.
- Assist patient only when necessary. Offer positive feedback for independent behavior.
- Rationale: Dependency on the nurse decreases self-esteem. Encouraging desired behaviors promotes effective coping.
- Encourage patient to make choices about his care.
- Rationale: Reduces helplessness and enhances sense of self-esteem.
- Identify expectations from patients for behavior and what consequences will occur if limits are not honed.
- Rationale: Helps set boundaries for manipulative behavior. Manipulation by the patient reduces sense of insecurity by increasing feeling of power.
- Assist patient to identify behavior and accept responsibility for actions.
- Rationale: A sense of responsibility needs to be developed before any changes can occur.
- Identify patient’s positive qualities and accomplishments and assist patient to recognize these traits.
- Rationale: Patient will have less need for manipulative behavior if self-esteem is increased.
- Congratulate the patient when he or she uses effective coping strategies.
- Rationale: Helps reinforce positive behavior.
- Encourage patient to utilize community resources, support systems, counselors, and family and friends.
- Rationale: Helps to maintain effective coping skills.
- Instruct patient/family in appropriate coping strategies.
- Rationale: Provides knowledge and identifies alternatives to inappropriate behavior.
- Instruct patient and/or family regarding need for support groups and/or counseling.
- Rationale: May be required to continue complete appropriate care and enable patient to effectively maintain coping skills.
Nursing Diagnosis
Deficient Knowledge
May be related to
- lack of knowledge about Parkinson’s disease
- stigma of disease
- difficulty understanding the disease process
- lack of coping skills
- cognitive impairment
Possibly evidenced by
- verbalization of questions
- verbalization of incorrect information
- noncompliant
- presence of preventable complications
- inability to follow instructions
- inappropriate behavior
- agitation
- depression
- withdrawal
- apathy
- restlessness
Desired Outcomes
- Patient and/or family will be able to exhibit understanding of disease process, medication regimen, and treatment plan of care.
- Patient will be able to accurately verbalize understanding of parkinsonism and its treatment regimen.
- Patient will be able to comply with medication regimen and notify physician if patient experiences untoward side effects.
- Patient and/or family will be able to identify and demonstrate safety precautions to prevent injury.
- Patient and/or family will be able to identify need for long-term goals and potential for end-of-life decisions to be made.
Nursing Interventions
- Assess patient’s understanding of disease process. Consider the older patient’s life experiences.
- Rationale: Provides baseline of understanding from which to establish a plan of care. New information can be used the patient’s existing knowledge base and life experience.
- Educate patient and/or SO about Parkinson’s disease, signs and symptoms, treatments and prevention of complications. Limit length of teaching sessions and provide quiet and productive environment for each session.
- Rationale: Elderly patients may not be aware of old information and the stigma that was attached to PD and dementia, and will require re-education regarding current treatments. Reduction of extraneous stimuli assists with learning and the ability to process new information without distraction. Short sessions allow patient to learn at own speed and prevent information overload.
- Prepare patient for surgery as indicated.
- Rationale: Surgical options may be required to replenish dopamine, improve dyskinesias and rigidity, or to treat disabling drug-resistant tremors.
- Advise the patient to take the anti-parkinsonism drugs on schedule.
- Rationale: The patient can adjust the schedule to produce peak effect of the drug when mobility is mostly needed.
- Instruct patient and/or SO regarding medications and need for compliance with dosage, scheduling, and physician follow-up.
- Rationale: Provides knowledge and facilitates compliance with treatment regimen. Provides for timely identification of serious adverse effect from medication regimen to allow physician to be notified postdischarge from hospital.
- Instruct family regarding side effects of medications and when to notify the physician.
- Rationale:
- Anticholinergic drugs (diphenhydramine, trihexyphenidyl, procyclidine) can cause sedation, confusion, and urinary retention.
- Dopaminergic drugs (carbidopa-levodopa) can cause nausea, anorexia, confusion, psychotic disturbances, dyskinesia, and nightmares.
- Dopamine agonists (bromocriptine) can cause nausea, vomiting, confusion, hallucination, dyskinesia and hypotension.
- MAOIs (selegiline) can cause nausea, insomnia, and confusion.
- Amantadine can cause urinary retention, increased intraocular pressure, and confusion.
- Rationale:
- Provide time for questions and concerns to be voiced, and answer questions honestly. Give patient and/or family written materials to refer to later.
- Rationale: Provide for correction of misinformation and written materials allow for documentation to assist with care once patient is discharged.
- Instruct patient and/or family regarding need for long-term planning and potential for end-of-life care decisions.
- Rationale: Disease is chronic and patient will eventually become severely impaired. Issues that may occur in the future (tube feedings, DNR, etc) should be discussed to enable patient and family to make informed choices while the patient is capable of understanding the severity of the condition.

