Notes
Description
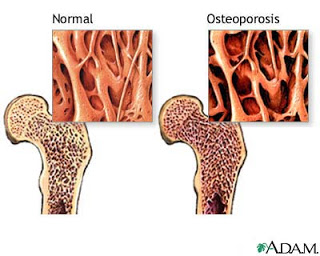
- Osteoporosis is an age-related metabolic disease that is defined as low bone mass with a normal ratio of mineral to osteoid, the organic matrix of bone.

- Bone demineralization results in the loss of bone mass, leading to fragile and porous bones and subsequent fractures.
- Greater bone resorption than bone formation occurs
- Occurs most commonly in the wrist, hip, and vertebral column.
- Osteoporosis can occur postmenopausally or as a result of a metabolic disorder or calcium deficiency.
- Client may be asymptomatic until the bones become so weak that a sudden injury causes a fracture.
Causes
- The exact cause of osteoporosis is unknown. A mild but prolonged negative calcium balance, resulting from an inadequate dietary intake of calcium, may be an important contributing factor.
- Declining gonadal adrenal function, faulty protein metabolism because of estrogen deficiency, and a sedentary lifestyle may also contribute. Risk factors that increase the likelihood of osteoporosis also include smoking, advanced age, heavy caffeine consumption, vitamin D deficiency, excess alcohol consumption, long-term heparin or corticosteroid use, and the use of laxatives or antacids. In addition, patients who are postmenopausal are more susceptible to osteoporosis.
- Patients who have Cushing’s disease or Parkinson’s disease, rheumatoid arthritis, scoliosis, or anorexia or who have had bilateral oophorectomy are also at greater risk. Paradoxically, both a sedentary lifestyle and excessive exercise are thought to be risk factors for osteoporosis.
Risk Factors
Modifiable
- Cigarette smoking
- Excessive use of alcohol
- Insufficient intake of calcium
- Sedentary lifestyle
Non- modifiable
- Early menopause
- Family history
- Female gender
- Increasing age
- Thin, small frame
- White (European descent) or Asian race
Assessment
- Possibly asymptomatic
- Back pain after lifting, bending, or stooping
- Back pain that increases with palpation
- Pelvic or hip pain, especially with weight bearing
- Problems with balance
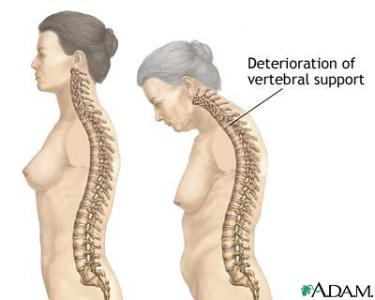
- Decline in height from venebral compression
- Kyphosis of the dorsal spine.
- Constipation, abnormal distention, and respiratory impairment as a result of movement restriction and spinal deformity
- Pathological fractures
- Appearance of thin, porous bone on x-ray film.
Primary Nursing Diagnosis
- Pain (acute) related to fracture
Diagnostic Evaluation
- Bone mineral density (BMD) reported as a T-score:
- (Osteopenia: T-score of –1 to –2.5 SD Osteoporosis: T-score of <–2.5 SD Severe osteoporosis: T-score of <–2.5 SD with fragility fracture(s)). BMD is the best predictor of fracture risk.
- Dual energy x-ray absorptiometry (DXA) reveals bone loss >3%.
- Bone x-rays shows bone loss( cannot determine bone loss until 25%–40% has occurred).
- Other Tests: Complete blood count, chemistry screening, thyroid-stimulating hormone level, urinalysis, serum protein electrophoresis, serum and urine calcium levels, vitamin D level, serum phosphorus levels, alkaline phosphatase, computed tomography (CT) scan
Medical Management
- Adequate, balanced diet rich in calcium and vitamin D
- Increased calcium intake in adolescents and elderly, or prescribe a calcium supplement with meals or beverages high in vitamin C.
- Regular weight-bearing exercise to promote bone formation (20-30 minutes aerobic exercises 3 days/week)
- Other medications; the bisphosphonates alendronate (Fosamax), risedronate (Actonel), and ibandronate, selective receptor modulators (SERMs), raloxifene (Evista), calcitonin
Pharmacologic Highlights
- Calcium supplements (1000–1500 mg/day PO; 1500 recommended for postmenopausal women and men over 50) to prevent bone loss and supplements calcium.
- Alendronate (Fosamax) [Bone resorption inhibitor; similar preparations with different doses are risedronate (Actonel),etidronate (Didronel),and ibandronate (BONIVA)] to prevent bone loss and inhibits bone resorption.
- Estrogen hormone such as conjugated estrogen (Provera) is given to prevent bone loss and reduces number of fractures; needs to be initiated within 3–5 yr of menopause; long-term therapy is no longer recommended when menopausal symptoms abate.
- Other Drugs: Androgens, calcitonin, and vitamin D metabolites may be ordered to decrease bone resorption. Analgesics may also be needed to manage the pain.
Nursing Interventions
- Assess risk for injury.
- Provide a safe and hazard-free environment, and assist the client to identify hazards in the home environment.
- Use side rails to prevent falls.
- Move the client gently when turning and repositioning.
- Encourage ambulation; assist with ambulation if the client is unsteady.
- Instruct in the use of assistive devices such as a cane or walker.
- Provide range of motion exercises.
- Instruct the client in the use of good body mechanics.
- Instruct the client in exercises to strengthen abdominal and back muscles to improve posture and provide support for the spine.
- Instruct the client to avoid activities that can cause vertebral compression.
- Apply a back brace as prescribed during an acute phase to immobilize the spine and provide spinal column support.
- Encourage the use of a firm mattress.
- Provide a diet high in protein, calcium, vitamins C, D and iron.
- Encourage adequate fluid intake to prevent calculuses.
- Advise the client to avoid alcohol and coffee.
- Administer estrogen or androgens to decrease the rate of bone resorption as prescribed.
- Administer calcium, vitamin D, and phosphorus as prescribed for bone metabolism.
- Administer calcitonin as prescribed to inhibit bone loss.
- Administer analgesics, muscle relaxants, and anti-inflammatory medications as prescribed.
Documentation Guidelines
- Physical findings of musculoskeletal assessment: Pain, mobility, numbness, curvature of the spine
- Response to pain medications
- Reaction to exercise plan and orthotic devices
Discharge and Home Healthcare Guidelines
- Reinforce the medication, exercise, and diet plan.
- Provide a hazard-free environment to prevent falls. Apply orthotic devices correctly. Remove scatter rugs, provide good lighting, and install handrails in the bathroom.
- Be sure the patient understands all medications, including the dosage, route, action, and side effects. If the patient is placed on estrogen therapy, she needs routine gynecologic checkups to detect early signs of cervical cancer.
- Consider placement in a nursing home if a patient cannot return home. Communicate the special needs of the patient on the transfer chart. The need for physical or occupational therapy, social work, and homemaking personnel is determined by the home care nurse. Facilitate the procurement of needed orthotic devices or ambulation aids before the patient goes home. The Osteoporosis Foundation provides information to clients regarding the disease and its treatment.
Exam
Nursing Care Plan
Nursing Diagnosis
Impaired Physical Mobility
May be related to
- Bone loss
- Pain
- Fracture
- Inability to bear weight
Possibly evidenced by
- Spontaneous fracture
Desired Outcomes
- Patient will maintain functional mobility as long as possible within limitations of disease process.
- Patient will have a few, if any, complications related to immobility as disease condition progresses
Nursing Interventions
- Assess patient’s functional ability for mobility and note changes.
- Rationale: Identifies problems and helps to establish a plan of care.
- Provide range of motion exercises every shift. Encourage active range of motion exercises.
- Rationale: Helps to prevent joint contractures and muscle atrophy.
- Reposition patient every 2 hours and prn.
- Rationale: Turning at regular intervals prevents skin breakdown from pressure injury.
- Apply trochanter rolls and/or pillows to maintain joint alignment.
- Rationale: Prevents musculoskeletal deformities.
- Assist patient with walking if at all possible, utilizing sufficient help. A one or two-person pivot transfer utilizing a transfer belt can be used if patient has weight-bearing ability.
- Rationale: Preserves patient’s muscle tone and helps prevent complications of immobility.
- Use mechanical lift for patients who cannot bear weight, and help them out of bed at least daily.
- Rationale: Provides change of scenery, movement, and encourages participation in activities.
- Avoid restraints as possible.
- Rationale: Inactivity created by the use of restraints may increase muscle weakness and poor balance.
- Instruct family regarding ROM exercises, methods of transferring patients from bed to wheelchair, and turning at routine intervals.
- Rationale: Prevents complications of immobility and knowledge assists family members to be better prepared for home care.
- Assess degree of immobility produced by injury or treatment and note patient’s perception of immobility.
- Rationale: Patient may be restricted by self-view or self-perception out of proportion with actual physical limitations, requiring information or interventions to promote progress toward wellness.
- Encourage participation in diversional or recreational activities. Maintain stimulating environment (radio, TV, newspapers, personal possessions, pictures, clock, calendar, visits from family and friends).
- Rationale: Provides opportunity for release of energy, refocuses attention, enhances patient’s sense of self-control and self-worth, and aids in reducing social isolation.
- Instruct patient or assist with active and passive ROM exercises of affected and unaffected extremities.
- Rationale: Increases blood flow to muscles and bone to improve muscle tone, maintain joint mobility; prevent contractures or atrophy and calcium resorption from disuse
- Encourage use of isometric exercises starting with the unaffected limb.
- Rationale: Isometrics contract muscles without bending joints or moving limbs and help maintain muscle strength and mass. Note: These exercises are contraindicated while acute bleeding and edema is present.
- Provide footboard, wrist splints, trochanter or hand rolls as appropriate.
- Rationale: Useful in maintaining functional position of extremities, hands and feet, and preventing complications (contractures, footdrop).
- Place in supine position periodically if possible, when traction is used to stabilize lower limb fractures.
- Rationale: Reduces risk of flexion contracture of hip.
- Instruct and encourage use of trapeze and “post position” for lower limb fractures.
- Rationale: Facilitates movement during hygiene or skin care and linen changes; reduces discomfort of remaining flat in bed. “Post position” involves placing the uninjured foot flat on the bed with the knee bent while grasping the trapeze and lifting the body off the bed.
- Assist with self-care activities (bathing, shaving).
- Rationale: Improves muscle strength and circulation, enhances patient control in situation, and promotes self-directed wellness.
- Provide and assist with mobility by means of wheelchair, walker, crutches, canes as soon as possible. Instruct in safe use of mobility aids.
- Rationale: Early mobility reduces complications of bed rest (phlebitis) and promotes healing and normalization of organ function. Learning the correct way to use aids is important to maintain optimal mobility and patient safety.
- Monitor blood pressure (BP) with resumption of activity. Note reports of dizziness.
- Rationale: Postural hypotension is a common problem following prolonged bed rest and may require specific interventions (tilt table with gradual elevation to upright position).
- Reposition periodically and encourage coughing and deep-breathing exercises.
- Rationale: Prevents or reduces incidence of skin and respiratory complications (decubitus, atelectasis, pneumonia).
- Auscultate bowel sounds. Monitor elimination habits and provide for regular bowel routine. Place on bedside commode, if feasible, or use fracture pan. Provide privacy.
- Rationale: Bed rest, use of analgesics, and changes in dietary habits can slow peristalsis and produce constipation. Nursing measures that facilitate elimination may prevent or limit complications. Fracture pan limits flexion of hips and lessens pressure on lumbar region and lower extremity cast.
- Encourage increased fluid intake to 2000–3000 mL per day (within cardiac tolerance), including acid or ash juices.
- Rationale: Keeps the body well hydrated, decreasing risk of urinary infection, stone formation, and constipation
- Provide diet high in proteins, carbohydrates, vitamins, and minerals, limiting protein content until after first bowel movement.
- Rationale: In the presence of musculoskeletal injuries, nutrients required for healing are rapidly depleted, often resulting in a weight loss of as much as 20 to 30 lb during skeletal traction. This can have a profound effect on muscle mass, tone, and strength. Note: Protein foods increase contents in small bowel, resulting in gas formation and constipation. Therefore, gastrointestinal (GI) function should be fully restored before protein foods are increased.
- Increase the amount of roughage or fiber in the diet. Limit gas-forming foods.
- Rationale: Adding bulk to stool helps prevent constipation. Gas-forming foods may cause abdominal distension, especially in presence of decreased intestinal motility.
- Consult with physical, occupational therapist or rehabilitation specialist.
- Rationale: Useful in creating individualized activity and exercise program. Patient may require long-term assistance with movement, strengthening, and weight-bearing activities, as well as use of adjuncts (walkers, crutches, canes); elevated toilet seats; pickup sticks or reachers; special eating utensils.
- Initiate bowel program (stool softeners, enemas, laxatives) as indicated.
- Rationale: Done to promote regular bowel evacuation.
- Refer to psychiatric clinical nurse specialist or therapist as indicated.
- Rationale: Patient or SO may require more intensive treatment to deal with reality of current condition, prognosis, prolonged immobility, perceived loss of control.
Nursing Diagnosis
Imbalanced Nutrition: Less Than Body Requirements
May be related to
- Inadequate calcium and vitamin D
Possibly evidenced by
- Deformity
- Kyphosis
- Loss of height
- Fractures
Desired Outcomes
- Patient will demonstrate adequate intake of calcium and vitamin D.
Nursing Interventions
- Instruct recommended daily intake for calcium.
- Rationale: Premenopausal women (19-50 years old) need 1,500 mg of calcium daily. After menopause, the requirement is 1,200 mg daily. Getting enough vitamin D is equally important as getting enough calcium because vitamin D aids in absorption of calcium and improves muscle strength.
- Instruct on the importance of adequate exposure to sunlight to prevent vitamin D deficiency.
- Rationale: The patient should be outside 15 minutes daily.
- If patient has limited exposure to sunlight, encourage vitamin D supplementation.
- Rationale: Supplementation will ensure adequate vitamin D intake.
- Instruct patient to perform gentle exercises.
- Rationale: Exercise can help build strong bones and slow bone loss. Strength-training exercises should be combined with weight-bearing exercises. Strength training helps in bone and muscle strength.
- Limit alcohol intake
- Rationale: Consuming more than two alcoholic drinks a day may decrease bone formation and reduce the body’s ability to absorb calcium.
- Provide a balanced diet.
- Rationale: A diet high in nutrients that support skeletal metabolism: vitamin D, calcium, and protein.
- Limit caffeine intake
- Rationale: Limit the amount of caffeinated beverages to about two to three cups of coffee a day. As long as the diet contains adequate calcium, moderation in caffeine consumption won’t harm the patient. Note also caffeine-containing beverages like colas and some teas.
Nursing Diagnosis
Risk for Poisoning
May be related to
- Drug toxicity, interactions with prescribed medications
- Polypharmacy
- Analgesic abuse
- Physiologic changes associated with the aging process
- Cognitive limitations
Possibly evidenced by
- Usage of numerous medications
- Adverse medicine effects
- Drug toxicity levels
- Inability to take medication correctly
- Pain
- Use of analgesic in doses sufficient to cause toxicity or interact with other medicines
- Disorientation
- Impaired vision
- Multiple health care providers
- Multiple pharmacies
- Inability to understand drug interactions or usage
Desired Outcomes
- Patient will be able to prescribed medications in correct quantities at correct times, and will not exhibit signs or symptoms of drug interaction or toxicity.
- Patient will be able to accurately verbalize understanding of need for one medical provider to control care.
- Patient and/or family will be able to accurately verbalize understanding of all medications, their effects, side effects, and potential drug interactions.
- Patient and/or family will be compliant with providing safe environment for the patient by keeping medications in a secure location.
- Patient will be able to accurately verbalize understanding of appropriate medication administration.
- Patient will exhibit no signs or symptoms of drug toxicity, or suffer problems with drug interactions.
Nursing Interventions
- Evaluate the patient’s entire collection of medications, including over-the-counter drugs, vitamin and mineral supplements, herbal remedies, and dietary regimen.
- Rationale: Provides information as to what drugs and substances are being utilized concurrently and what drug interactions may occur with concurrent use, as well as with dietary consumption. Incorrect administration of medications to be taken on an empty stomach may cause inhibition of the appropriate action of the drug. Concurrent use of other medications can result in potentiation of action and create drug toxicity.
- Encourage patient and/or family to utilize one primary doctor to coordinate care.
- Rationale: Prevents utilization of several physicians who are unaware of each other’s treatment regimens and may duplicate medication or prescribe medication that may affect other drugs.
- Administer drugs as ordered, being cognizant of any interactions that might be possible.
- Rationale: Most of the time, elderly patients are on several medications, and the medicines used in treatment of osteoporosis can interact with other drugs, causing either a decrease or potentiation of other action.
- Provide instructions for use of medications, quantity, frequency, number of doses and times, and under what conditions they are to be taken.
- Rationale: Facilitates understanding of medication regimen and provides reference material once patient is discharged.
- Ensure medication labels are inscribed in large print with dosage instructions.
- Rationale: Prevents medication errors for patients with visual impairments.
- Assist patient and/or family to establish a system of following medication regimen accurately, such as use of calendars, charts, medication boxes that are labeled for each day of the week, and so forth.
- Rationale: Assists in reduction of medication errors and assists family to be involved in patient’s care.
- Discuss medications with physician about potential for using alternative long-acting drugs that require only one daily dosage.
- Rationale: May help to decrease the number of medications per day and simplify the patient’s regimen and facilitate compliance.
- Monitor lab work for toxicity levels, imbalances of electrolytes and other factors pertinent to patient’s medication profile.
- Rationale: Helps to reduce risk of toxicity. Age-related changes in the body, such as renal or liver impairment, decrease metabolism of drugs, so what may be considered a normal dosage may become toxic for patient with impaired function.
- Instruct patient/family regarding all medications, their use, effects and side-effects, and adverse reactions that should be reported to the physician.
- Rationale: Helps to promote knowledge and facilitates compliance.
- Instruct patient and/or family to store drugs in a secure area away from the bedside.
- Rationale: Elderly patients may have some memory loss, forgetting that they’ve already taken medicine, and double the dose taken. Frequently, elderly patients keep their medications in their bedside table to prevent the need to get up at night.
- Instruct patient and/or family regarding interactions that may occur with concurrent medication usage.
- Rationale: SERMS decreases the action of anticoagulants and ampicillin; bisphosphonates can result in hypercalcemia; estrogens can decrease the action of anticoagulants and oral hypoglycemics, and other drugs; calcium can decrease the action of estrogens.
Nursing Diagnosis
Deficient Knowledge
May be related to
- Lack of exposure to information regarding medications, dietary modifications, or safe activity program.
Possibly evidenced by
- Verbalization of the problem and request for information
- Fear of further bone loss and fractures
- Presence of preventable complication
Desired Outcomes
- Patient will achieve increased knowledge and compliance with medical regimen to minimize bone demineralization and injury.
- Patient will be compliant with medication and dietary instructions.
- Patient will be able to perform daily exercises within identified limitations and to prevent further bone loss or deterioration.
- Patient will exhibit no injury, fall, or trauma that might predispose to a fracture.
- Patient will be independent in performing ADLs with modifications.
- Patient and/or family will be able to accurately verbalize understanding of medications and methods of administration.
Nursing Interventions
- Assess patient’s knowledge of disease, diet, medication, and exercise program to arrest progression of of bone deterioration.
- Rationale: Provides basis for teaching and techniques to promote compliance. Disease is not usually detected until 24-40% of calcium in bone is lost.
- Assess the patient’s understanding of osteoporosis.
- Rationale: Most individuals with osteoporosis are not diagnosed until an acute fracture occurs.
- Provide support for body image and lifestyle changes.
- Rationale: Assists patient to cope with chronicity of disease and potential fractures causing pain and immobility.
- Assist to plan exercise program according to capabilities; to avoid flexion of spine and wear corset if appropriate (walking is preferred to jogging).
- Rationale: Exercise will strengthen bone. Vertebral collapse is common and corset provides support.
- Teach patient about nutrition and calcium intake.
- Rationale: Adequate calcium helps to prevent osteoporosis in women with small frame, increased age, Asians, and Caucasians.
- Teach the patient that calcium carbonate is most effective form of calcium.
- Rationale: Calcium carbonate is best absorbed in an acidic stomach. Adults 19-50 years of age should take 1000mg of elemental calcium daily and individuals 51 years above should take 1,200 mg daily.
- Instruct patient that vitamin D supplementation is indicated for patients with limited sun exposure.
- Rationale: Vitamin D supplements are needed for people living in the extreme northern or southern latitudes with limited sun exposure. Recommended vitamin D is 200 IU through age 50; 400 IU for 51-70 year olds, and 600 IU for >70 yr.
- Instruct patient in methods to perform activities of daily living and to avoid lifting, bending, or carrying heavy objects.
- Rationale: Prevents injury that can occur with osteoporosis with minimal trauma.
- Instruct patient and/or family in administration of calcium, vitamin D, estrogens, and other drug therapy for osteoporosis.
- Rationale: Provides replacement of calcium and helps to decrease bone loss.
- Instruct patient about medication for osteoporosis, adverse effects, administration, and need for follow-up tests.
- Rationale: An informed patient is likely to adhere to the medication regimen and report adverse effects.
- Instruct patient and/or family regarding potential referrals to therapy as warranted.
- Rationale: May help to provide exercise and the development of an activity program to maintain bone condition and encourage independence in ADLs.
- Teach patient and/or family regarding the use of assistive devices and safety precautions that are that are available to maintain mobility.
- Rationale: Prevents further trauma or fractures from falls resulting from lack of support.
- Administer and teach patient about the following drugs: alendronate (Fosamax), risedronate (Actonel), ibandronate (Boniva), or zoledronate (Reclast)
- Rationale:
- Bisphosphonates inhibit the activity of osteoclasts.
- Risedronate may be taken once daily or weekly.
- Ibandronate requires only monthly administration.
- Zoledronate is given IV once yearly.
- Oral bisphosphonates must be taken on first rising, without eating or drinking for 30 mins.
- Rationale:
- Administer and teach patient about raloxifene (Evista)
- Rationale: Evista is a selective estrogen receptor modulator; it has positive effects on bone mineral density and can be taken at any time of day.
- Instruct patient about weight bearing exercises.
- Rationale: Weight-bearing exercise contributes to increase bone density and prevents bone loss.
Other Nursing Care Plan


