Notes
Description
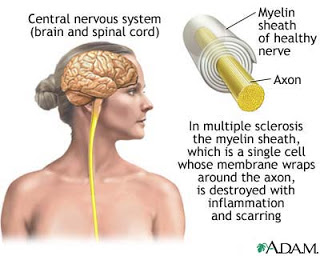
- Multiple sclerosis is a chronic, progressive, non- contagious, degenerative disease of the CNS characterized by demyelinization of the neurons.

- Multiple sclerosis usually occurs between the ages of 20 and 40 and consists of periods of remissions and exacerbations.
- The causes are unknown, but the disease is thought to be a result of an autoimmune response or viral infection.
- Precipitating factors include pregnancy, fatigue, stress, infection, and trauma.
- Electroencephalogram findings are abnormal
- A lumbar puncture indicates increased gamma globulin, but the serum globulin level is normal.
Causes
The cause of MS is unknown. Some evidence suggests that an infective agent causes a predisposition to MS, although that agent has not been identified. Some evidence supports immunologic, environmental, or genetic factors as possible causes of the disease. The risk of developing MS is 15 times higher when the disease is present in the patient’s immediate family. Conditions such as pregnancy, infection, and trauma seem to precipitate the onset of MS or cause relapses
Assessment
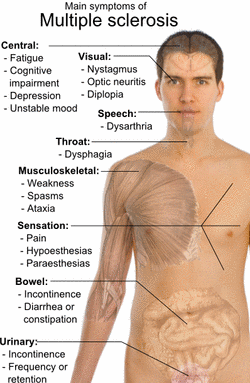
- Fatigue and weakness
- Ataxia and vertigo
- Tremors and spasticity of the lower extremities
- Parasthesias
- Blurred vision and diplopia
- Nystagmus
- Dysphasia
- Decreased perception to pain, touch, and temperature
- Bladder and bowel disturbances, including urgency, frequency, retention, and incontinence
- Abnormal reflexes, including hyperreflexia, absent reflexes, and a positive Babinski’s reflex
- Emotional changes such as apathy, euphoria, irritability, and depression
- Memory changes and confusion
Primary Nursing Diagnosis
- Impaired physical mobility related to fatigue and weakness.
Diagnostic Evaluation
- Cerebrospinal fluid (CSF) analysis reveals elevated protein level, increased white blood cells. Electrophoresis of CSF shows increased myelin basic protein and IgG bands.
- Other Tests: No single test reliably diagnoses MS. Supporting tests include electroencephalography, evoked potential studies, computed tomography (CT) scan, and magnetic resonance imaging (MRI).
Medical Management
- Most medical treatment is designed to slow disease progression and address the symptoms of the disease, such as urinary retention, spasticity, and motor and speech deficits. Currently, however, physicians generally prescribe steroid therapy to reduce tissue edema during an acute exacerbation.
- Consult with a physical therapist if the patient needs to learn how to use assistive devices or needs to learn exercises to maintain muscle tone and joint mobility.
- Muscle stretching for spastic muscles and selective strengthening exercises for weakness are prescribed.
- A social service agency may be required to help the family deal with the often expensive and long-term financial effect of the disease. Vocational redirection may also be required.
- For a patient who is experiencing depression, consider a referral to a psychiatric clinical nurse specialist. Family counseling is often very helpful.
Pharmacologic Highlights
- Corticosteroids agents, such as Prednisone (Orasone); methylprednisolone or (Solu-Medrol); dexamethasone(Decadron) maybe used to help decrease symptoms and induce remissions through anti-inflammatory effects.
- Immunomodulatory agents, such as Interferon, cyclosporine, azathioprine, methotrexate maybe used to help decrease symptoms and induce remissions; treatment includes combination therapy using two or more of these agents.
- Other Drugs: Antianxiety agents, such as chlordiazepoxide hydrochloride (Librium), may be prescribed to manage mood swings; baclofen (Lioresal) or dantrolene (Dantrium) may be used to relieve muscle spasticity; and patients with urinary symptoms may require behanechol (Urecholine) or oxybutynin (Ditropan).
Nursing Interventions
- Provide bed rest during exacerbation.
- Protect the client from injury by providing safety measures.
- Place an eye patch on the eye for diplopia.
- Monitor for potential complications such as urinary tract infections, calculuses, decubitus ulcers, respiratory tract infections, and contractures.
- Promote regular elimination by bladder and bowel training.
- Encourage independence.
- Assist the client to establish a regular exercise and rest program.
- Instruct the client to balance moderate activity with rest periods.
- Assess the need for and provide assistive devices.
- Initiate physical and speech therapy.
- Instruct the client to avoid fatigue, stress, infection, overheating, and chilling.
- Instruct the client to increase fluid intake and eat a balanced diet, including low-fat, high-fiber foods and foods high in potassium.
- Instruct the client in safety measures related to sensory loss, such as regulating the temperature of bath water and avoiding heating pads.
- Instruct the client in safety measures related to motor loss, such as avoiding the use of scatter rugs and using assistive devices.
- Instruct the client in the self-administration of prescribed medications.
- Provide information about the National Multiple Sclerosis Society.
Documentation Guidelines
- Physical findings; Muscle strength, gait, muscle symmetry, visual response
- Response to medications, treatments, and special therapies
- Ability to perform self-care, bowel and bladder care
- Presence of complications, infections, contractures
Discharge and Home Healthcare Guidelines
- Be sure the patient understands any pain medication prescribed, including dosage, route, action, and side effects.
- Be sure the patient understands the need for adequate bladder and bowel elimination.
- Instruct the patient to notify the primary caregiver of any exacerbation or sudden worsening of the condition.
- If the patient has difficulty speaking or communicating, be sure that she or he has access to a telephone support network or some other means of calling for assistance when she or he is at home alone for any length of time.
- Be sure the patient understands that stress, fatigue, and being overheated stimulate exacerbations. Teach the patient how to avoid situations that produce these reactions. Be sure the patient knows how to contact community agencies such as the MS Society for use of such in-home equipment as beds and wheelchairs and home maintenance support.
- Determine whether a home care agency is needed to provide home supervision and ongoing physical therapy support.
Exam
[mtouchquiz 602 title=off]
Nursing Care Plan
Nursing Diganosis
Fatigue
May be related to
- Decreased energy production, increased energy requirements to perform activities
- Psychological/emotional demands
- Pain/discomfort
- Medication side effects
Possibly evidenced by
- Verbalization of overwhelming lack of energy
- Inability to maintain usual routines; decreased performance
- Impaired ability to concentrate; disinterest in surroundings
- Increase in physical complaints
Desired Outcomes
- Identify risk factors and individual actions affecting fatigue.
- Identify alternatives to help maintain desired activity level.
- Participate in recommended treatment program.
- Report improved sense of energy.
Nursing Interventions
- Note and accept presence of fatigue.
- Rationale: Fatigue is the most persistent and common symptom of MS. Studies indicate that the fatigue encountered by patients with MS occurs with expenditure of minimal energy, is more frequent and severe than “normal” fatigue, has a disproportionate impact on ADLs, has a slower recovery time, and may show no direct relationship between fatigue severity and patient’s clinical neurological status.
- Identify and review factors affecting ability to be active: temperature extremes, inadequate food intake, insomnia, use of medications, time of day.
- Rationale: Provides opportunity to problem-solve to maintain or improve mobility.
- Accept when patient is unable to do activities.
- Rationale: Ability can vary from moment to moment. Nonjudgmental acceptance of patient’s evaluation of day-to-day variations in capabilities provides opportunity to promote independence while supporting fluctuations in level of required care.
- Determine need for walking aids. Provide braces, walkers, or wheelchairs. Review safety considerations.
- Rationale: Mobility aids can decrease fatigue, enhancing independence and comfort, as well as safety. However, individual may display poor judgment about ability to safely engage in activity.
- Schedule ADLs in the morning if appropriate. Investigate use of cooling vest.
- Rationale: Fatigue commonly worsens in late afternoon (when body temperature rises). Some patients report lessening of fatigue with stabilization of body temperature.
- Plan care consistent rest periods between activities. Encourage afternoon nap.
- Rationale: Reduces fatigue, aggravation of muscle weakness.
- Assist with physical therapy. Increase patient comfort with massages and relaxing baths.
- Rationale: Reduces fatigue and promotes sense of wellness.
- Stress need for stopping exercise or activity just short of fatigue.
- Rationale: Pushing self beyond individual physical limits can result in excessive or prolonged fatigue and discouragement. In time, patient can become very adept at knowing limitations.
- Investigate appropriateness of obtaining a service dog.
- Rationale: Service dogs can increase patient’s level of independence. They can also assist in energy conservation by carrying items in “saddle” bags and retrieving or performing tasks.
- Recommend participation in groups involved in fitness or exercise and/or the Multiple Sclerosis Society.
- Rationale: Can help patient to stay motivated to remain active within the limits of the disability or condition. Group activities need to be selected carefully to meet patient’s needs and prevent discouragement or anxiety.
Administer medications as indicated:
- Amantadine (Symmetrel); pemoline (Cylert)
- Rationale: Useful in treatment of fatigue. Positive antiviral drug effect in 30%–50% of patients. Use may be limited by side effects of increased spasticity, insomnia, paresthesias of hands and feet.
- Methylphenidate (Ritalin), modafinil (Provigil)
- Rationale: CNS stimulants that may reduce fatigue but may also cause side effects of nervousness, restlessness, and insomnia.
- Sertraline (Zoloft), fluoxetine (Prozac)
- Rationale: Antidepressants useful in lifting mood, and “energizing” patient (especially when depression is a factor) and when patient is free of anticholinergic side effects.
- Tricyclic antidepressants: amitriptyline (Elavil), nortriptyline (Pamelor)
- Rationale: Useful in treating emotional lability, neurogenic pain, and associated sleep disorders to enhance willingness to be more active.
- Anticonvulsants: carbamazepine (Tegretol), gabapentin (Neurontin), lamotrigine (Lamictal)
- Rationale: Used to treat neurogenic pain and sudden intermittent spasms related to spinal cord irritation.
- Steroids: prednisone (Deltasone), dexamethasone (Decadron), methyl-prednisolone (Solu-Medrol)
- Rationale: May be used during acute exacerbations to reduce and prevent edema formation at the sclerotic plaques. Note: Long-term therapy seems to have little effect on progression of symptoms.
- Vitamin B
- Rationale: Supports nerve-cell replication, enhances metabolic functions, and may increase sense of well-being and energy level.
- Immuno-modulating agents: cyclo phosphamide (Cytoxan), azathioprine (Imuran), methotrexate (Mexate), interferon [beta]-1B (Betaseron); interferon [beta]-1A (Avonex, Rebif), glatiramer (Copaxone); mitoxantrone (Novantrone).
- Rationale: May be used to treat acute relapses, reduce the frequency of relapse, and promote remission. Interferon [beta]-1B (Betaseron) has been approved for use by ambulatory patients with remitting relapsing MS and is the first drug found to alter the course of the disease. Current research indicates early treatment with drugs that reduce inflammation and lesion formation may limit permanent damage. Therapy of choice is “A, B, C” drugs: Avonex, Betaseron, and Copaxone. Therapeutic benefits have been reported in patients at all stages of disability with reduction in both steroid use and hospital days. (Copaxone chemically resembles a component of myelin and may act as a decoy, diverting immune cells away from myelin target.) Note: Novantrone may be used if other medications not effective but is contraindicated in patients with primary progressive MS.
- Prepare for plasma exchange treatment as indicated.
- Rationale: Research suggests that individuals experiencing severe exacerbations not responding to standard therapy may benefit from a course of plasma exchange
Nursing Diagnosis
Self-care Deficit
May be related to
- Neuromuscular/perceptual impairment; intolerance to activity; decreased strength and endurance; motor impairment, tremors
- Pain, discomfort, fatigue
- Memory loss
- Depression
Possibly evidenced by
- Frustration; inability to perform tasks of self-care, poor personal hygiene
Desired Outcomes
- Identify individual areas of weakness/needs.
- Demonstrate techniques/lifestyle changes to meet self-care needs.
- Perform self-care activities within level of own ability.
- Identify personal/community resources that provide assistance.
Nursing Interventions
- Determine current activity level and physical condition. Assess degree of functional impairment using 0–4 scale.
- Rationale: Provides information to develop plan of care for rehabilitation. Note: Motor symptoms are less likely to improve than sensory ones.
- Encourage patient to perform self-care to the maximum of ability as defined by patient. Do not rush patient.
- Rationale: Promotes independence and sense of control; may decrease feelings of helplessness.
- Assist according to degree of disability; allow as much autonomy as possible.
- Rationale: Participation in own care can ease the frustration over loss of independence.
- Encourage patient input in planning schedule.
- Rationale: Patient’s quality of life is enhanced when desires and likes are considered in daily activities.
- Note presence of fatigue.
- Rationale: Fatigue experienced by patients with MS can be very debilitating and greatly impact ability to participate in ADLs. The subjective nature of reports of fatigue can be misinterpreted by healthcare providers and family, leading to conflict and the belief that the patient is “manipulative” when, in fact, this may not be the case.
- Encourage scheduling activities early in the day or during the time when energy level is best.
- Rationale: Patients with MS expend a great deal of energy to complete ADLs, increasing the risk of fatigue, which often progresses through the day.
- Allot sufficient time to perform tasks, and display patience when movements are slow.
- Rationale: Decreased motor skills and spasticity may interfere with ability to manage even simple activities.
- Anticipate hygienic needs and calmly assist as necessary with care of nails, skin, and hair; mouth care; shaving.
- Rationale: Caregiver’s example can set a matter-of-fact tone for acceptance of handling mundane needs that many be embarrassing to patient and repugnant to SO.
- Provide assistive devices and aids as indicated: shower chair, elevated toilet seat with arm supports.
- Rationale: Reduces fatigue, enhancing participation in self-care.
- Reposition frequently when patient is immobile (bed or chair bound). Provide skin care to pressure points, such as sacrum, ankles, and elbows. Position properly and encourage to sleep prone as tolerated.
- Rationale: Reduces pressure on susceptible areas, prevents skin breakdown. Minimizes flexor spasms at knees and hips.
- Provide massage and active or passive ROM exercises on a regular schedule. Encourage use of splints or footboards as indicated.
- Rationale: Prevents problems associated with muscle dysfunction and disuse. Helps maintain muscle tone and strength and joint mobility, and decreases risk of loss of calcium from bones.
- Encourage stretching and toning exercises and use of medications, cold packs, and splints and maintenance of proper body alignment, when indicated.
- Rationale: Helps decrease spasticity and its effects.
- Problem-solve ways to meet nutritional and fluid needs.
- Rationale: Provides for adequate intake and enhances patient’s feelings of independence or self-esteem.
- Consult with physical and/or occupational therapist.
- Rationale: Useful in identifying devices and/or equipment to relieve spastic muscles, improve motor functioning, prevent and reduce muscular atrophy and contractures, promoting independence and increasing sense of self-worth.
Administer medications as indicated:
- Tizanidine (Zanaflex), baclofen (Lioresal), carbamazepine (Tegretol);
- Rationale: Newer drugs used for reducing spasticity, promoting muscle relaxation, and inhibiting reflexes at the spinal nerve root level. Enhance mobility and maintenance of activity. Tizanidine (Zanaflex) may have an additive effect with baclofen (Lioresal), but use with caution because both drugs have similar side effects. Short duration of action requires careful individualizing of dosage to maximize therapeutic effect.
- Diazepam (Valium), clonazepam (Klonopin), cyclobenzaprine (Flexeril), gabapentin (Neurontin, dantrolene (Dantrium);
- Rationale: A variety of medications are used to reduce spasticity. The mechanisms are not well understood, and responses vary in each person. Therefore, it may take a period of medication trials to discover what provides the most effective relief of muscle spasticity and associated pain. Note: Adverse effects may be increased muscle weakness, loss of muscle tone, and liver toxicity.
- Meclizine (Antivert), scopolamine patches (Transderm-Scop).
- Rationale: Reduces dizziness, allowing patient to be more mobile.
Nursing Diagnosis
Low Self-Esteem
May be related to
- Change in structure/function
- Disruption in how patient perceives own body
- Role reversal; dependence
Possibly evidenced by
- Confusion about sense of self, purpose, direction in life
- Denial, withdrawal, anger
- Negative/self-destructive behavior
- Use of ineffective coping methods
- Change in self/other’s perception of role/physical capacity to resume role
Desired Outcomes
- Verbalize realistic view and acceptance of body as it is.
- View self as a capable person.
- Participate in and assume responsibility for meeting own needs.
- Recognize and incorporate changes in self-concept/role without negating self-esteem.
- Develop realistic plans for adapting to role changes.
Nursing Interventions
- Establish and maintain a therapeutic nurse-patient relationship, discussing fears and concerns.
- Rationale: Conveys an attitude of caring and develops a sense of trust between patient and caregiver in which patient is free to express fears of rejection, loss of previous functioning and/or appearance, feelings of helplessness, powerlessness about changes that may occur. Promotes a sense of well-being for patient.
- Note withdrawn behaviors and use of denial or over concern with body and disease process.
- Rationale: Initially may be a normal protective response, but if prolonged, may prevent dealing appropriately with reality and may lead to ineffective coping.
- Support use of defense mechanisms, allowing patient to deal with information in own time and way.
- Rationale: Confronting patient with reality of situation may result in increased anxiety and lessened ability to cope with changed self-concept/role.
- Acknowledge reality of grieving process related to actual or perceived changes. Help patient deal realistically with feelings of anger and sadness.
- Rationale: Nature of the disease leads to ongoing losses and changes in all aspects of life, blocking resolution of grieving process.
- Review information about course of disease, possibility of remissions, prognosis.
- Rationale: When patient learns about disease and becomes aware that own behavior (including feeling hopeful/ maintaining a positive attitude) can significantly improve general well-being and daily functioning, patient may feel more in control, enhancing sense of self-esteem. Note: Some patients may never have a remission.
- Provide accurate verbal and written information about what is happening and discuss with patient/SO.
- Rationale: Helps patient stay in the “here and now,” reduces fear of the unknown; provides reference source for future use.
- Explain that labile emotions are not unusual. Problem-solve ways to deal with these feelings.
- Rationale: Relieves anxiety and assists with efforts to manage unexpected emotional displays.
- Note presence of depression and impaired thought processes, expressions of suicidal ideation (evaluate on a scale of 1–10).
- Rationale: Adapting to a long-term, progressively debilitating incurable disease is a difficult emotional adjustment. In addition, cognitive impairment may affect adaptation to life changes. A depressed individual may believe that suicide is the best way to deal with what is happening.
- Assess interaction between patient and SO. Note changes in relationship.
- Rationale: SO may unconsciously or consciously reinforce negative attitudes and beliefs of patient, or issues of secondary gain may interfere with progress and ability to manage situation.
- Provide open environment for patient and SO to discuss concerns about sexuality, including management of fatigue, spasticity, arousal, and changes in sensation.
- Rationale: Physical and psychological changes often create stressors within the relationship, affecting usual roles and expectations, further impairing self-concept.
- Discuss use of medications and adjuncts to improve sexual function.
- Rationale: Patient and partner may want to explore trial of medications (papaverine [Pavabid], dinoprostone [Prostin E2]) or other avenues of improving sexual relationship.
- Consult with occupational therapist/ rehabilitation team.
- Rationale: Identifying assistive devices and/or equipment enhances level of overall function and participation in activities, enhancing sense of well-being and viewing self as a capable individual.
Nursing Diagnosis
Powerlessness/Hopelessness
May be related to
- Illness-related regimen, unpredictability of disease
- Lifestyle of helplessness
Possibly evidenced by
- Verbal expressions of having no control or influence over situation
- Depression over physical deterioration that occurs despite patient compliance with regimen
- Nonparticipation in care or decision making when opportunities are provided
- Passivity, decreased verbalization/affect
- Verbal cues
- Lack of involvement in care/passively allowing care
- Isolating behaviors/social withdrawal
Desired Outcomes
- Identify and verbalize feelings.
- Use coping mechanisms to counteract feelings of hopelessness.
- Identify areas over which individual has control.
- Participate/monitor and control own self-care and ADLs within limits of the individual situation.
Nursing Interventions
- Note behaviors indicative of powerlessness or hopelessness. Patient may say statements of despair.
- Rationale: The degree to which patient believes own situation is hopeless, that he or she is powerless to change what is happening, affects how patient handles life situation.
- Acknowledge reality of situation, at the same time expressing hope for patient.
- Rationale: Although the prognosis may be discouraging, remissions may occur, and because the future cannot be predicted, hope for some quality of life should be encouraged. Additionally, research is ongoing and new treatment options are being initiated.
- Encourage and assist patient to identify activities he or she would like to be involved in within the limits of his or her abilities.
- Rationale: Staying active and interacting with others counteract feelings of helplessness.
- Discuss plans for the future. Suggest visiting alternative care facilities, taking a look at the possibilities for care as condition changes.
- Rationale: When options are considered and plans are made for any eventuality, patient has a sense of control over own circumstances.
- Determine degree of mastery patient has exhibited in life to the present. Note locus of control.
- Rationale: Patient who has assumed responsibility in life previously tends to do the same during difficult times of exacerbation of illness. However, if locus of control has been focused outward, patient may blame others and not take control over own circumstances.
- Assist patient to identify factors that are under own control. List things that can or cannot be controlled.
- Rationale: Knowing and accepting what is beyond individual control can reduce helpless or acting out behaviors, promote focusing on areas individual can control.
- Encourage patient to assume control over as much of own care as possible.
- Rationale: Even when unable to do much physical care, individual can help plan care, having a voice in what is desired or not.
- Discuss needs openly with patient/SO, setting up agreed-on routines for meeting identified needs.
- Rationale: Helps deal with manipulative behavior, when patient feels powerless and not listened to.
- Incorporate patient’s daily routine into home care schedule or hospital stay, as possible.
- Rationale: Maintains sense of control and self-determination and independence.
- Refer to vocational rehabilitation as indicated.
- Rationale: Can assist patient to develop and implement a vocational plan incorporating specific interests and/or abilities.
- Identify community resources.
- Rationale: Participation in structured activities can reduce sense of isolation and may enhance feeling of self-worth.
Nursing Diagnosis
Risk for Ineffective Coping
Risk factors may include
- Physiological changes (cerebral and spinal lesions)
- Psychological conflicts; anxiety; fear
- Impaired judgment, short-term memory loss; confusion; unrealistic perceptions/ expectations, emotional lability
- Personal vulnerability; inadequate support systems
- Multiple life changes
- Inadequate coping methods
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired Outcomes
- Recognize relationship between disease process (cerebral lesions) and emotional responses, changes in thinking/behavior.
- Verbalize awareness of own capabilities/strengths.
- Display effective problem-solving skills.
- Demonstrate behaviors/lifestyle changes to prevent/minimize changes in mentation and maintain reality orientation.
Nursing Interventions
- Assess current functional capacity and limitations; note presence of distorted thinking processes, labile emotions, cognitive dissonance. Note how these affect the individual’s coping abilities.
- Rationale: Organic or psychological effects may cause patient to be easily distracted, to display difficulties with concentration, problem solving, dealing with what is happening, being responsible for own care.
- Determine patient’s understanding of current situation and previous methods of dealing with life’s problems.
- Rationale: Provides a clue as to how patient may deal with what is currently happening, and helps identify individual resources and need for assistance.
- Discuss ability to make decisions, care for children or dependent adults, handle finances. Identify options available to individuals involved.
- Rationale: Impaired judgment, confusion, inadequate support systems may interfere with ability to meet own needs and needs of others. Conservatorship, guardianship, or adult protective services may be required until (if ever) patient is able to manage own affairs.
- Maintain an honest, reality-oriented relationship.
- Rationale: Reduces confusion and minimizes painful, frustrating struggles associated with adaptation to altered environment or lifestyle.
- Encourage verbalization of feelings and/or fears, accepting what patient says in a nonjudgmental manner. Note statements reflecting powerlessness, inability to cope.
- Rationale: May diminish patient’s fear, establish trust, and provide an opportunity to identify problems and begin the problem-solving process.
- Observe nonverbal communication: posture, eye contact, movements, gestures, and use of touch. Compare with verbal content and verify meaning with patient as appropriate.
- Rationale: May provide significant information about what patient is feeling; however, verification is important to ensure accuracy of communication. Discrepancy between feelings and what is being said can interfere with ability to cope, problem-solve.
- Provide clues for orientation: calendars, clocks, notecards, organizers.
- Rationale: These serve as tangible reminders to aid recognition and permeate memory gaps and enable patient to cope with situation.
- Encourage patient to tape-record important information and listen to the recording periodically.
- Rationale: Repetition puts information in long-term memory, where it is more easily retrieved and can support decision-making and problem-solving process.
- Refer to cognitive retraining program.
- Rationale: Improving cognitive abilities can enhance basic thinking skills when attention span is short; ability to process information is impaired; patient is unable to learn new tasks; or insight, judgment, and problem-solving skills are impaired.
- Refer to counseling, psychiatric clinical nurse specialist and/or psychiatrist, as indicated.
- Rationale: May need additional help to resolve issues of self-esteem and regain effective coping skills.
- Administer medications as appropriate: amitriptyline (Elavil); bupropion (Wellbutrin); imipramine (Tofranil);
- Rationale: Medications to improve mood and restful sleep may be useful in combating depression and relieving degree of fatigue interfering with function.
Nursing Diagnosis
Ineffective Family Coping
May be related to
- Situational crisis; temporary family disorganization and role changes
- Highly ambivalent family relationship
- Prolonged disease/disability progression that exhausts the supportive capacity of SO
- Patient providing little support in turn for SO
- SO with chronically unexpressed feelings of guilt, anxiety, hostility, despair
Possibly evidenced by
- Patient expresses/confirms concern or complaint about SO response to patient’s illness
- SO withdraws or has limited personal communication with patient or displays protective behavior disproportionate to patient’s abilities or need for autonomy.
- SO preoccupied with own personal reactions
- Intolerance, abandonment
- Neglectful care of patient
- Distortion of reality regarding patient’s illness
Desired Outcomes
- Identify/verbalize resources within themselves to deal with the situation.
- Express more realistic understanding and expectations of patient.
- Interact appropriately with patient/healthcare providers providing support and assistance as indicated.
- Verbalize knowledge and understanding of disability/disease and community resources.
Nursing Interventions
- Note length, severity of illness. Determine patient’s role in family and how illness has changed the family organization.
- Rationale: Chronic illness, accompanied by changes in role performance and responsibility, often exhausts supportive capacity and coping abilities of SO or family.
- Determine SO’s understanding of disease process and expectations for the future.
- Rationale: Inadequate information and misconception regarding disease process and/or unrealistic expectations affect ability to cope with current situation. Note: A particular area of misconception is the fatigue experienced by patients with MS. Family members may view patient’s inability to perform activities as manipulative behavior rather than an actual physiological deficit.
- Discuss with SO/family members their willingness to be involved in care. Identify other responsibilities and factors impacting participation.
- Rationale: Individuals may not have desire or time to assume responsibility for care. If several family members are available, they may be able to share tasks.
- Assess other factors that are affecting abilities of family members to provide needed support.
- Rationale: Individual members’ preoccupation with own needs and concerns can interfere with providing needed care and support for stresses of long-term illness. Additionally, caregiver(s) may incur decrease or loss of income or risk losing own health insurance if they alter their work hours.
- Discuss underlying reasons for patient’s behaviors.
- Rationale: Helps SO understand and accept and deal with behaviors that may be triggered by emotional or physical effects of MS.
- Encourage patient and SO to develop and strengthen problem-solving skills to deal with situation.
- Rationale: Family may or may not have handled conflict well before illness, and stress of long-term debilitating condition can create additional problems (including unresolved anger).
- Encourage free expression of feelings, including frustration, anger, hostility, and hopelessness.
- Rationale: Individual members may be afraid to express “negative” feelings, believing it will discourage patient. Free expression promotes awareness and can help with resolution of feelings and problems (especially when done in a caring manner).
- Identify community resources and local MS organization, support groups, home care agencies, respite programs.
- Rationale: Provides information, opportunities to share with others who are experiencing similar difficulties, and sources of assistance when needed.
- Refer to social worker, financial adviser, psychiatric clinical nurse specialist and psychiatrist as appropriate.
- Rationale: May need more in-depth assistance from professional sources.
Nursing Diagnosis
Impaired Urinary Elimination
May be related to
- Neuromuscular impairment (spinal cord lesions/neurogenic bladder)
Possibly evidenced by
- Incontinence; nocturia; frequency
- Retention with overflow
- Recurrent UTIs
Desired Outcomes
- Verbalize understanding of condition.
- Demonstrate behaviors/techniques to prevent/minimize infection.
- Empty bladder completely and regularly (voluntarily or by catheter as appropriate).
- Be free of urine leakage.
Nursing Interventions
- Note reports of urinary frequency, urgency, burning, incontinence, nocturia, and size or force of urinary stream. Palpate bladder after voiding.
- Rationale: Provides information about degree of interference with elimination or may indicate bladder infection. Fullness over bladder following void is indicative of inadequate emptying or retention and requires intervention.
- Review drug regimen, including prescribed, over-the-counter (OTC), and street.
- Rationale: A number of medications such as some antispasmodics, antidepressants, and narcotic analgesics; OTC medications with anticholinergic or alpha agonist properties; or recreational drugs such as cannabis may interfere with bladder emptying.
- Institute bladder training program or timed voidings as appropriate.
- Rationale: Helps restore adequate bladder functioning; lessens occurrence of incontinence and bladder infection.
- Encourage adequate fluid intake, avoiding caffeine and use of aspartame, and limiting intake during late evening and at bedtime. Recommend use of cranberry juice/ vitamin C.
- Rationale: Sufficient hydration promotes urinary output and aids in preventing infection. Note: When patient is taking sulfa drugs, sufficient fluids are necessary to ensure adequate excretion of drug, reducing risk of cumulative effects. Note: Aspartame, a sugar substitute (e.g., Nutrasweet), may cause bladder irritation leading to bladder dysfunction.
- Promote continued mobility.
- Rationale: Decreases risk of developing UTI.
- Recommend good hand washing and proper perineal care.
- Rationale: Reduces skin irritation and risk of ascending infection.
- Encourage patient to observe for sediments or blood in urine, foul odor, fever, or unexplained increase in MS symptoms.
- Rationale: Indicative of infection requiring further evaluation or treatment.
- Refer to urinary continence specialist as indicated.
- Rationale: Helpful for developing individual plan of care to meet patient’s specific needs using the latest techniques, continence products.
Administer medications as indicated:
- Oxybutynin (Ditropan), propantheline (Pro-Banthine), hyoscyamine sulfate (Cytospaz-M), flavoxate hydrochloride (Urispas), tolterodine (Detrol).
- Rationale: Reduce bladder spasticity and associated symptoms of frequency, urgency, incontinence, nocturia.
- Catheterize as indicated.
- Rationale: May be necessary as a treatment and for evaluation if patient is unable to empty bladder or retains urine.
- Teach self-catheterization and instruct in use and care of indwelling catheter.
- Rationale: Helps patient maintain autonomy and encourages self-care. Indwelling catheter may be required, depending on patient’s abilities and degree of urinary problem.
- Obtain periodic urinalysis and urine culture and sensitivity as indicated.
- Rationale: Monitors renal status. Colony count over 100,000 indicates presence of infection requiring treatment.
Administer anti-infective agents as necessary:
- Nitrofurantoin macrocrystals. (Macrodantin); co-trimoxazole (Bactrim, Septra); ciprofloxacin (Cipro); norfloxacin (Noroxin).
- Rationale: Bacteriostatic agents that inhibit bacterial growth and destroy susceptible bacteria. Prompt treatment of infection is necessary to prevent serious complications of sepsis/shock
Nursing Diagnosis
Knowledge Deficit
May be related to
- Lack of exposure; information misinterpretation
- Unfamiliarity with information resources
- Cognitive limitation, lack of recall
Possibly evidenced by
- Statement of misconception
- Request of information
- Inaccurate follow-through of instruction; development of preventable complications
- Inappropriate or exaggerated behaviors (e.g., hysterical, hostile, agitated, apathetic)
Desired Outcomes
- Participate in learning process.
- Assume responsibility for own learning and begin to look for information and to ask questions.
- Verbalize understanding of condition/disease process and treatment.
- Initiate necessary lifestyle changes.
- Participate in prescribed treatment regimen.
Nursing Interventions
- Evaluate desire and readiness of patient and SO and/or caregiver to learn.
- Rationale: Determines amount or level of information to provide at any given moment.
- Note signs of emotional lability or whether patient is in dissociative state (loss of affect, inappropriate emotional responses).
- Rationale: Patient will not process or retain information and will have difficulty learning during this time.
- Provide information in varied formats depending on patient’s cognitive or perceptual abilities and considering patient’s locus of control.
- Rationale: Changes in cognitive, visual, auditory function impact choice of teaching modalities: verbal instruction, books, pamphlets, audiovisuals, computer programs. Whether locus of control is internal or external affects patient’s attitude toward helpfulness of learning.
- Encourage active participation of patient or SO in learning process, including use of self-paced instruction as appropriate.
- Rationale: Enhances sense of independence and control and may strengthen commitment to therapeutic regimen.
- Review disease process or prognosis, effects of climate, emotional stress, overexertion, fatigue.
- Rationale: Clarifies patient or SO understanding of individual situation.
- Identify signs and symptoms requiring further evaluation.
- Rationale: Prompt intervention may help limit severity of exacerbation or complications.
- Discuss importance of daily routine of rest, exercise, activity, and eating, focusing on current capabilities. Instruct in use of appropriate devices to assist with ADLs, e.g., eating utensils, walking aids.
- Rationale: Helps patient maintain current level of physical independence and may limit fatigue.
- Stress necessity of weight control.
- Rationale: Excess weight can interfere with balance and motor abilities and make care more difficult.
- Review possible problems that may arise, such as decreased perception of heat and pain, susceptibility to skin breakdown and infections, especially UTI.
- Rationale: These effects of demyelination and associated complications may compromise patient safety and/or precipitate an exacerbation of symptoms.
- Identify actions that can be taken to avoid injury, e.g., avoid hot baths, inspect skin regularly, take care with transfers and wheelchair/ walker mobility, force fluids, and get adequate nutrition. Encourage avoidance of persons with upper respiratory infection.
- Rationale: Review of risk factors can help patient take measures to maintain physical state at optimal level/prevent complications.
- Discuss increased risk of osteoporosis and review preventive measures, e.g., regular exercise, intake of calcium and vitamin D, reduced intake of caffeine, cessation of smoking, hormone replacement therapy (HRT) or alternatives (e.g., bisphosphonates—Fosamax), and fall prevention measures such as wearing low-heeled shoes with nonskid soles, use of handrails/ grab bars in bathroom and along stairwells, removal of small area rugs.
- Rationale: Decreased mobility, vitamin D deficiency (possibly a result increased of decreased exposure to sunlight, which can exacerbate MS symptoms), and decreased likelihood of engaging in preventive measures increase bone mass loss and the risk of fractures.
- Identify bowel elimination concerns. Recommend adequate hydration and intake of fiber; use of stool softeners, bulking agents, suppositories, or possibly mild laxatives; bowel training program.
- Rationale: Constipation is common, and bowel urgency and/or accidents may occur as a result of dietary deficiencies or impaction.
- Review specifics of individual medications. Recommend avoidance of OTC drugs.
- Rationale: Reduces likelihood of drug interactions and/or adverse effects, and enhances cooperation with treatment regimen.
- Discuss concerns regarding sexual relationships, contraception and reproduction, effects of pregnancy on affected woman. Identify alternative ways to meet individual needs; counsel regarding use of artificial lubrication (females), genitourinary (GU) referral for males regarding available medication and sexual aids.
- Rationale: Pregnancy may be an issue for the young patient relative to issues of genetic predisposition and/or ability to manage pregnancy or parent offspring. Increased libido is not uncommon and may require adjustments within the existing relationship or in the absence of an acceptable partner. Information about different positions and techniques and/or other options for sexual fulfillment (e.g., fondling, cuddling) may enhance personal relationship and feelings of self-worth.
- Encourage patient to set goals for the future while focusing on the “here and now,” what can be done today.
- Rationale: Having a plan for the future helps retain hope and provides opportunity for patient to see that although today is to be lived, one can plan for tomorrow even in the worst of circumstances.
- Identify financial concerns.
- Rationale: Loss or change of employment (for patient and/or SO) impacts income, insurance benefits, and level of independence, requiring additional family and social support.
- Refer for vocational rehabilitation as appropriate.
- Rationale: May need assessment of capabilities and job retraining as indicated by individual limitations and disease progression.
- Recommend contacting local and national MS organizations, relevant support groups.
- Rationale: Ongoing contact (e.g., mailings) informs patient of programs and services available, and can update patient’s knowledge base. Support groups can provide role modeling, sharing of information and enhance problem-solving ability.
Nursing Diagnosis
Risk for Caregiver Role Strain
Risk factors may include
- Severity of illness of the care receiver, duration of caregiving required,
- complexity/amount of caregiving task
- Caregiver is female, spouse
- Care receiver exhibits deviant, bizarre behavior
- Family/caregiver isolation; lack of respite and recreation
Desired Outcomes
- Identify individual risk factors and appropriate interventions.
- Demonstrate/initiate behaviors or lifestyle changes to prevent development of impaired function.
- Use available resources appropriately.
- Report satisfaction with plan and support available.
Nursing Interventions
- Note physical/mental condition, therapeutic regimen of care receiver.
- Rationale: Determines individual needs for planning care. Identifies strengths and how much responsibility patient may be expected to assume, as well as disabilities requiring accommodation.
- Determine caregiver’s level of commitment, responsibility, involvement in and anticipated length of care. Use assessment tool, such as Burden Interview, to further determine caregiver’s abilities, when appropriate.
- Rationale: Progressive debilitation taxes caregiver and may alter ability to meet patient or own needs.
- Discuss caregiver’s view of and about situation.
- Rationale: Allows ventilation and clarification of concerns, promoting understanding.
- Determine available supports and resources currently used.
- Rationale: Organizations can provide information regarding adequacy of supports and identify needs.
- Facilitate family conference to share information and develop plan for involvement in care activities as appropriate.
- Rationale: When others are involved in care, the risk of one person’s becoming overloaded is lessened.
- Identify additional resources to include financial, legal assistance.
- Rationale: These areas of concern can add to burden of caregiving if not adequately resolved.
- Identify adaptive equipment needs and resources for the home and vehicles.
- Rationale: Enhances independence and safety of both caregiver and patient.
- Provide information and/or demonstrate techniques for dealing with acting-out or violent or disoriented behavior.
- Rationale: Helps caregiver maintain sense of control and competency. Enhances safety for care receiver and caregiver.
- Stress importance of self-nurturing: pursuing self-development interests, personal needs, hobbies, and social activities.
- Rationale: Taking time for self can lessen risk of “burnout”/being overwhelmed by situation.
- Identify alternate care sources (such as sitter or day care facility), senior care services, home care agency.
- Rationale: As patient’s condition worsens, SO may need additional help from several sources to maintain patient at home even on a part-time basis.
- Assist caregiver to plan for changes that may be necessary for the care receiver (eventual placement in extended care facility).
- Rationale: Planning for this eventually is important for the time when burden of care becomes too great.
- Refer to supportive services as need indicates.
- Rationale: Medical case manager or social services consultant may be needed to develop ongoing plan to meet changing needs of patient and SO/family.
Other Possible Nursing Care Plans
- Trauma, risk for—weakness, poor vision, balancing difficulties, reduced temperature/tactile sensation, reduced muscle and hand/eye coordination, cognitive or emotional difficulties, insufficient finances to purchase necessary equipment.
- Home Maintenance, impaired—insufficient finances, unfamiliarity with neighborhood resources, inadequate support systems.
- Disuse Syndrome, risk for/[actual]—paralysis/immobilization, severe pain.
- Therapeutic Regimen: ineffective management—economic difficulties, family conflict, social support deficits.
