Notes
Description
- Hypertension, or high blood pressure (BP), is defined as a persistent systolic blood pressure (SBP) greater than or equal to 140 mm Hg, diastolic blood pressure (DBP) greater than or equal to 90 mm Hg, or current use of antihypertensive medication. There is a direct relationship between hypertension and cardiovascular disease (CVD).
- Contributing factors to the development of hypertension include cardiovascular risk factors combined with socioeconomic conditions and ethnic differences.
- Hypertension is generally an asymptomatic condition. Individuals who remain undiagnosed and untreated for hypertension present the greatest challenge and opportunity for health care providers.
- Is the most important modifiable risk factor for stroke.
- High blood pressure increases the risk of ischemic heart disease by 3-4 fold
- The incidence of stroke increases approximately 8 fold in persons with definite hypertension
- It has been estimated that 40% of cases of acute MI or stroke are attributable to hypertension
Etiology of Hypertension
- Primary (essential or idiopathic) hypertension: elevated BP without an identified cause; accounts for 90% to 95% of all cases of hypertension.
- Secondary hypertension: elevated BP with a specific cause; accounts for 5% to 10% of hypertension in adults.
Pathophysiology
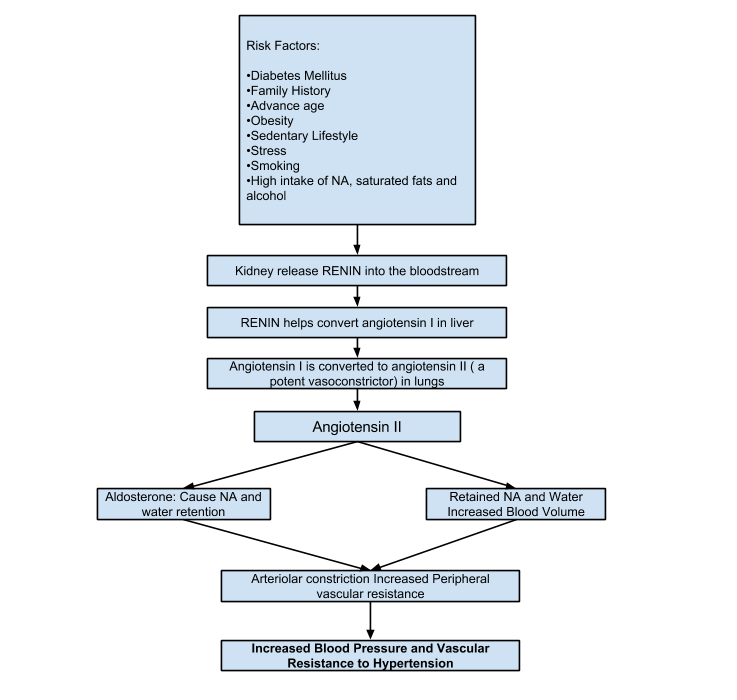
PATHOPHYSIOLOGY OF PRIMARY HYPERTENSION
- The hemodynamic hallmark of hypertension is persistently increased SVR.
- Water and sodium retention: A high-sodium intake may activate a number of pressor mechanisms and cause water retention.
- Altered renin-angiotensin mechanism: High plasma renin activity (PRA) results in the increased conversion of angiotensinogen to angiotensin I causing arteriolar constriction, vascular hypertrophy, and aldosterone secretion.
- Stress and increased SNS activity: Arterial pressure is influenced by factors such as anger, fear, and pain. Physiologic responses to stress, which are normally protective, may persist to a pathologic degree, resulting in prolonged increase in SNS activity. Increased SNS stimulation produces increased vasoconstriction, increased HR, and increased renin release.
- Insulin resistance and hyperinsulinemia: Abnormalities of glucose, insulin, and lipoprotein metabolism are common in primary hypertension. Additional pressor effects of insulin include vascular hypertrophy and increased renal sodium reabsorption.
- Endothelial cell dysfunction: Some hypertensive people have a reduced vasodilator response to nitric oxide. Nitric oxide, an endothelium-derived relaxing factor (EDRF), helps maintain low arterial tone at rest, inhibits growth of the smooth muscle layer, and inhibits platelet aggregation. Endothelin produces pronounced and prolonged vasoconstriction.
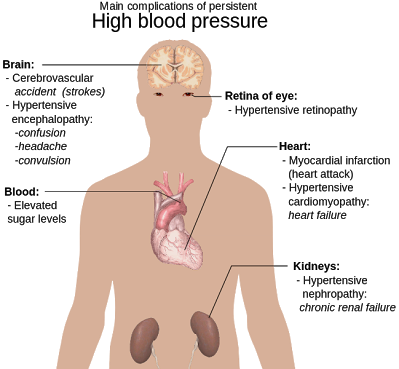
Clinical Manifestations of Hypertension
- Often called the “silent killer” because it is frequently asymptomatic until it becomes severe and target organ disease occurs.
- Target organ diseases occur in the heart (hypertensive heart disease), brain (cerebrovascular disease), peripheral vasculature (peripheral vascular disease), kidney (nephrosclerosis), and eyes (retinal damage).
- Hypertension is a major risk factor for coronary artery disease (CAD).
- Sustained high BP increases the cardiac workload and produces left ventricular hypertrophy (LVH). Progressive LVH, especially in association with CAD, is associated with the development of heart failure.
- Hypertension speeds up the process of atherosclerosis in the peripheral blood vessels, leading to the development of peripheral vascular disease, aortic aneurysm, and aortic dissection.
- Intermittent claudication (ischemic muscle pain precipitated by activity and relieved with rest) is a classic symptom of peripheral vascular disease involving the arteries.
- Hypertension is one of the leading causes of end-stage renal disease, especially among African Americans. The earliest manifestation of renal dysfunction is usually nocturia.
- The retina provides important information about the severity and duration of hypertension. Damage to retinal vessels provides an indication of concurrent vessel damage in the heart, brain, and kidney. Manifestations of severe retinal damage include blurring of vision, retinal hemorrhage, and loss of vision.
Classification of Hypertension: WHO/ISH*
| Category | Systolic | Diastolic |
| Optimal Normal High Normal |
< 120 <130 130-139 |
<80 <85 85-89 |
| Grade 1 (mild hypertension) – Subgroup: borderline |
140-159 140-149 |
90-99 90-94 |
| Grade 2 (moderate hypertension) | 160-179 | 100-109 |
| Grade 3 (severe Hypertension) | ≥ 180 | ≥110 |
| Isolated Systolic Hypertension (ISH) – Subgroup (borderline) |
≥140 140-149 |
<90 <90 |
| World Health Organization –ISH International Society of Hypertension | ||
National Institutes of Health Classification
| Category | Systolic | Diastolic |
| Optimal | < 120 | <80 |
| Pre-hypertensive | 120-139 | 80-89 |
| Hypertensive | ≥140 | ≥90 |
| Stage 1 | 140-159 | 90-99 |
| Stage 2 | ≥160 | ≥100 |
Diagnostic Studies
- Basic laboratory studies are performed to (1) identify or rule out causes of secondary hypertension, (2) evaluate target organ disease, (3) determine overall cardiovascular risk, or (4) establish baseline levels before initiating therapy.
- Routine urinalysis, BUN, serum creatinine, and creatinine clearance levels are used to screen for renal involvement and to provide baseline information about kidney function.
- Measurement of serum electrolytes, especially potassium levels, is done to detect hyperaldosteronism, a cause of secondary hypertension.
- Blood glucose levels assist in the diagnosis of diabetes mellitus.
- Lipid profile provides information about additional risk factors that predispose to atherosclerosis and cardiovascular disease.
- ECG and echocardiography provide information about the cardiac status.
Nursing and Collaborative Management
- Treatment goals are to lower BP to less than 140 mm Hg systolic and less than 90 mm Hg diastolic for most persons with hypertension (less than 130 mm Hg systolic and less than 80 mm Hg diastolic for those with diabetes mellitus and chronic kidney disease).
- Lifestyle modifications are indicated for all patients with prehypertension and hypertension and include the following:
- Weight reduction. A weight loss of 10 kg (22 lb) may decrease SBP by approximately 5 to 20 mm Hg.
- Dietary Approaches to Stop Hypertension (DASH) eating plan. Involves eating several servings of fish each week, eating plenty of fruits and vegetables, increasing fiber intake, and drinking a lot of water. The DASH diet significantly lowers BP.
- Restriction of dietary sodium to less than 6 g of salt (NaCl) or less than 2.4 g of sodium per day.
- This involves avoiding foods known to be high in sodium (e.g., canned soups) and not adding salt in the preparation of foods or at meals.
- Restriction of alcohol
- Regular aerobic physical activity (e.g., brisk walking) at least 30 minutes a day most days of the week. Moderately intense activity such as brisk walking, jogging, and swimming can lower BP, promote relaxation, and decrease or control body weight.
- It is strongly recommended that tobacco use be avoided.
- Stress can raise BP on a short-term basis and has been implicated in the development of hypertension. Relaxation therapy, guided imagery, and biofeedback may be useful in helping patients manage stress, thus decreasing BP.
Drug Therapy
- Drug therapy is not recommended for those persons with prehypertension unless it is required by another condition, such as diabetes mellitus or chronic kidney disease.
- The overall goals for the patient with hypertension include (1) achievement and maintenance of the goal BP; (2) acceptance and implementation of the therapeutic plan; (3) minimal or no unpleasant side effects of therapy; and (4) ability to manage and cope with illness.
- Drugs currently available for treating hypertension work by (1) decreasing the volume of circulating blood, and/or (2) reducing SVR.
- Diuretics promote sodium and water excretion, reduce plasma volume, decrease sodium in the arteriolar walls, and reduce the vascular response to catecholamines.
- Adrenergic-inhibiting agents act by diminishing the SNS effects that increase BP. Adrenergic inhibitors include drugs that act centrally on the vasomotor center and peripherally to inhibit norepinephrine release or to block the adrenergic receptors on blood vessels.
- Direct vasodilators decrease the BP by relaxing vascular smooth muscle and reducing SVR.
- Calcium channel blockers increase sodium excretion and cause arteriolar vasodilation by preventing the movement of extracellular calcium into cells.
- Angiotensin-converting enzyme (ACE) inhibitors prevent the conversion of angiotensin I to angiotensin II and reduce angiotensin II (A-II)–mediated vasoconstriction and sodium and water retention.
- A-II receptor blockers (ARBs) prevent angiotensin II from binding to its receptors in the walls of the blood vessels.
- Thiazide-type diuretics are used as initial therapy for most patients with hypertension, either alone or in combination with one of the other classes.
- When BP is more than 20/10 mm Hg above SBP and DBP goals, a second drug should be considered. Most patients who are hypertensive will require two or more antihypertensive medications to achieve their BP goals.
- Side effects and adverse effects of antihypertensive drugs may be so severe or undesirable that the patient does not comply with therapy.
- Hyperuricemia, hyperglycemia, and hypokalemia are common side effects with both thiazide and loop diuretics.
- ACE inhibitors lead to high levels of bradykinin, which can cause coughing. An individual who develops a cough with the use of ACE inhibitors may be switched to an ARB.
- Hyperkalemia can be a serious side effect of the potassium-sparing diuretics and ACE inhibitors.
- Sexual dysfunction may occur with some of the diuretics. Orthostatic hypotension and sexual dysfunction are two undesirable effects of adrenergic-inhibiting agents.
- Tachycardia and orthostatic hypotension are potential adverse effects of both vasodilators and angiotensin inhibitors.
- Patient and family teaching related to drug therapy is needed to identify and minimize side effects and to cope with therapeutic effects. Side effects may be an initial response to a drug and may decrease with continued use of the drug.
Hypertensive crisis
- Hypertensive crisis is a severe and abrupt elevation in BP, arbitrarily defined as a DBP more than 140 mm Hg.
- Hypertensive crisis occurs most often in patients with a history of hypertension who have failed to comply with their prescribed medications or who have been undermedicated.
- Hypertensive crisis related to cocaine or crack use is becoming a more frequent problem. Other drugs such as amphetamines, phencyclidine (PCP), and lysergic acid diethylamide (LSD) may also precipitate hypertensive crisis that may be complicated by drug-induced seizures, stroke, MI, or encephalopathy.
- Hypertensive emergency develops over hours to days and is defined as BP that is severely elevated (more than 180/120 mm Hg) with evidence of acute target organ damage.
- Hypertensive emergencies can precipitate encephalopathy, intracranial or subarachnoid hemorrhage, acute left ventricular failure with pulmonary edema, MI, renal failure, dissecting aortic aneurysm, and retinopathy.
- Hypertensive emergencies require hospitalization, intravenous (IV) administration of antihypertensive drugs, and intensive care monitoring.
Nursing Management
- The primary nursing responsibilities for long-term management of hypertension are to assist the patient in reducing BP and complying with the treatment plan. Nursing actions include patient and family teaching, detection and reporting of adverse treatment effects, compliance assessment and enhancement, and evaluation of therapeutic effectiveness.
- Patient and family teaching includes the following: (1) nutritional therapy, (2) drug therapy, (3) physical activity, (4) home monitoring of BP (if appropriate), and (5) tobacco cessation (if applicable).
Exam
Nursing Care Plan
Nursing Priorities
- Maintain/enhance cardiovascular functioning.
- Prevent complications.
- Provide information about disease process/prognosis and treatment regimen.
- Support active patient control of condition.
Nursing diagnosis: Risk for Decreased Cardiac Output
Risk factors may include
- Increased vascular resistance, vasoconstriction
- Myocardial ischemia
- Ventricular hypertrophy/rigidity
Possibly evidenced by
- not applicable; presence of signs and symptoms establishes an actual
Desired outcomes/evaluation criteria—patient will:
- Participate in activities that reduce blood pressure/cardiac workload.
- Maintain blood pressure within individually acceptable range.
- Demonstrate stable cardiac rhythm and rate within patient’s normal range.
Nursing Interventions
Hemodynamic regulation
Independent
- Monitor bp. Measure in both arms/thighs three times, 3–5 min apart while patient is at rest, then sitting, then standing for initial evaluation. Use correct cuff size and accurate technique.
- Rationale: Comparison of pressures provides a more complete picture of vascular involvement/scope of problem. Severe hypertension is classified in the adult as a diastolic pressure elevation to 110 mm hg; progressive diastolic readings above 120 mm hg are considered first accelerated, then malignant (very severe). Systolic hypertension also is an established risk factor for cerebrovascular disease and ischemic heart disease, when diastolic pressure is elevated.
- Note presence, quality of central and peripheral pulses.
- Rationale: Bounding carotid, jugular, radial, and femoral pulses may be observed/palpated. Pulses in the legs/feet may be diminished, reflecting effects of vasoconstriction increased systemic vascular resistance and venous congestion.
- Auscultate heart tones and breath sounds.
- Rationale: S4 heart sound is common in severely hypertensive patients because of the presence of atrial hypertrophy (increased atrial volume/pressure). Development of s3 indicates ventricular hypertrophy and impaired functioning. Presence of crackles, wheezes may indicate pulmonary congestion secondary to developing or chronic heart failure.
- Observe skin color, moisture, temperature, and capillary refill time.
- Rationale: Presence of pallor; cool, moist skin; and delayed capillary refill time may be due to peripheral vasoconstriction or reflect cardiac decompensation/decreased output.
- Note dependent/general edema.
- Rationale: May indicate heart failure, renal or vascular impairment.
- Provide calm, restful surroundings, minimize environmental activity/noise. Limit the number of visitors and length of stay.
- Rationale: Helps reduce sympathetic stimulation; promotes relaxation.
- Maintain activity restrictions, e.g., bedrest/chair rest; schedule periods of uninterrupted rest; assist patient with self-care activities as needed.
- Rationale: Reduces physical stress and tension that affect blood pressure and the course of hypertension.
- Provide comfort measures, e.g., back and neck massage, elevation of head.
- Rationale: Decreases discomfort and may reduce sympathetic stimulation.
- Instruct in relaxation techniques, guided imagery, distractions.
- Rationale: Can reduce stressful stimuli, produce calming effect, thereby reducing bp.
Medication
Independent
- Monitor response to medications to control blood pressure.
- Rationale: Response to drug therapy (usually consisting of several Drugs, including diuretics, angiotensin-converting enzyme [ace] inhibitors, vascular smooth muscle relaxants, beta and calcium channel blockers) is dependent on both the individual as well as the synergistic effects of the drugs.Because of side effects, drug interactions, and patient’s motivation for taking antihypertensive medication, it is important to use the smallest number and lowest dosage of medications.
Collaborative
- Administer medications as indicated: Thiazide diuretics, e.g., chlorothiazide (diuril); hydrochlorothiazide (esidrix/hydrodiuril); bendroflumethiazide (naturetin); indapamide (lozol); metolazone (diulo); quinethazone (hydromox);
- Rationale: Diuretics are considered first-line medications for uncomplicated stage i or ii hypertension and may be used alone or in association with other drugs (such as beta-blockers) to reduce bp in patients with relatively normal renal function. These diuretics potentiate the effects of other antihypertensive agents as well, by limiting fluid retention, and may reduce the incidence of strokes and heart failure.
- Loop diuretics, e.g., furosemide (lasix); ethacrynic acid (edecrin); bumetanide (bumex), torsemide (demadex)
- Rationale: These drugs produce marked diuresis by inhibiting resorption of sodium and chloride and are effective antihypertensives, especially in patients who are resistant to thiazides or have renal impairment.
- Potassium-sparing diuretics, e.g., spironolactone (aldactone); triamterene (dyrenium); amiloride (midamor)
- Rationale: May be given in combination with a thiazide diuretic to minimize potassium loss.
- Alpha, beta, or centrally acting adrenergic antagonists, e.g., doxazosin (cardura); propranolol (inderal); acebutolol (sectral); metoprolol (lopressor), labetalol (normodyne); atenolol (tenormin); nadolol (corgard), carvedilol (coreg); methyldopa (aldomet); clonidine (catapres); prazosin (minipress); terazosin (hytrin); pindolol (visken)
- Rationale: Beta-blockers may be ordered instead of diuretics for patients with ischemic heart disease; obese patients with cardiogenic hypertension; and patients with concurrent supraventricular arrhythmias, angina, or hypertensive cardiomyopathy. Specific actions of these drugs vary, but they generally reduce bp through the combined effect of decreased total peripheral resistance, reduced cardiac output, inhibited sympathetic activity, and suppression of renin release. Note: patients with diabetes should use corgard and visken with caution because they can prolong and mask the hypoglycemic effects of insulin. The elderly may require smaller doses because of the potential for bradycardia and hypotension. African-american patients tend to be less responsive to beta-blockers in general and may require increased dosage or use of another drug, e.g., monotherapy with a diuretic.
- Calcium channel antagonists, e.g., nifedipine (procardia); verapamil (calan); diltiazem (cardizem); amlodipine (norvasc); isradipine (dynacirc); nicardipine (cardene)
- Rationale: May be necessary to treat severe hypertension when a combination of a diuretic and a sympathetic inhibitor does not sufficiently control bp. Vasodilation of healthy cardiac vasculature and increased coronary blood flow are secondary benefits of vasodilator therapy.
- Adrenergic neuron blockers: guanadrel (hylorel); guanethidine (ismelin); reserpine (serpalan);
- Rationale: Reduce arterial and venous constriction activity at the sympathetic nerve endings.
- Direct-acting oral vasodilators: hydralazine (apresoline); minoxidil (loniten)
- Rationale: Action is to relax vascular smooth muscle, thereby reducing vascular resistance.
- Direct-acting parenteral vasodilators: diazoxide (hyperstat), nitroprusside (nitropress); labetalol (normodyne)
- Rationale: These are given intravenously for management of hypertensive emergencies.
- Angiotensin-converting enzyme (ace) inhibitors, e.g., captopril (capoten); enalapril (vasotec); lisinopril (zestril); fosinopril (monopril); ramipril (altace). Angiotensin ii blockers, e.g., valsartan (diovan), guanethidine (ismelin).
- Rationale: The use of an additional sympathetic inhibitor may be required for its cumulative effect when other measures have failed to control bp or when congestive heart failure (chf) or diabetes is present.
- Implement dietary sodium, fat, and cholesterol restrictions as indicated.
- Rationale: These restrictions can help manage fluid retention and, with associated hypertensive response, decrease myocardial workload.
- Prepare for surgery when indicated.
- Rationale: When hypertension is due to pheochromocytoma, removal of the tumor will correct condition
Nursing diagnosis: Activity Intolerance
May be related to
- Generalized weakness
- Imbalance between oxygen supply and demand
Possibly evidenced by
- Verbal report of fatigue or weakness
- Abnormal heart rate or bp response to activity
- Exertional discomfort or dyspnea
- Electrocardiogram (ecg) changes reflecting ischemia; dysrhythmias
Desired outcomes/evaluation criteria—patient will:
- Participate in necessary/desired activities.
- Report a measurable increase in activity tolerance.
- Demonstrate a decrease in physiological signs of intolerance.
Nursing Interventions
Energy Management
Independent
- Assess the patient’s response to activity, noting pulse rate more than 20 beats/min faster than resting rate; marked increase in bp during/after activity (systolic pressure increase of 40 mm hg or diastolic pressure increase of 20 mm hg); dyspnea or chest pain; excessive fatigue and weakness; diaphoresis; dizziness or syncope.
- Rationale: The stated parameters are helpful in assessing physiological responses to the stress of activity and, if present, are indicators of overexertion.
- Instruct patient in energy-conserving techniques, e.g., using chair when showering, sitting to brush teeth or comb hair, carrying out activities at a slower pace.
- Rationale: Energy-saving techniques reduce the energy expenditure, thereby assisting in equalization of oxygen supply and demand.
- Encourage progressive activity/self-care when tolerated. Provide assistance as needed.
- Rationale: Gradual activity progression prevents a sudden increase in cardiac workload. Providing assistance only as needed encourages independence in performing activities.
Nursing diagnosis: Acute Pain, Headache
May be related to
- Increased cerebral vascular pressure
Possibly evidenced by
- Reports of throbbing pain located in suboccipital region, present on awakening and disappearing spontaneously after being up and about
- Reluctance to move head, rubbing head, avoidance of bright lights and noise, wrinkled brow, clenched fists
- Reports of stiffness of neck, dizziness, blurred vision, nausea, and vomiting
Desired outcomes/evaluation criteria—patient will:
- Report pain/discomfort is relieved/controlled.
- Verbalize methods that provide relief.
- Follow prescribed pharmacological regimen
Nursing Interventions
Pain management
Independent
- Determine specifics of pain, e.g., location, characteristics, intensity (0–10 scale), onset/duration. Note nonverbal cues.
- Rationale: Facilitates diagnosis of problem and initiation of appropriate therapy. Helpful in evaluating effectiveness of therapy.
- Encourage/maintain bedrest during acute phase.
- Rationale: Minimizes stimulation/promotes relaxation.
- Provide/recommend nonpharmacological measures for relief of headache, e.g., cool cloth to forehead; back and neck rubs; quiet, dimly lit room; relaxation techniques (guided imagery, distraction); and diversional activities.
- Rationale: Measures that reduce cerebral vascular pressure and that slow/block sympathetic response are effective in relieving headache and associated complications.
- Eliminate/minimize vasoconstricting activities that may aggravate headache, e.g., straining at stool, prolonged coughing, bending over.
- Rationale: Activities that increase vasoconstriction accentuate the headache in the presence of increased cerebral vascular pressure.
- Assist patient with ambulation as needed.
- Rationale: Dizziness and blurred vision frequently are associated with vascular headache. Patient may also experience episodes of postural hypotension, causing weakness when ambulating.
- Provide liquids, soft foods, frequent mouth care if nosebleeds occur or nasal packing has been done to stop bleeding.
- Rationale: Promotes general comfort. Nasal packing may interfere with swallowing or require mouth breathing, leading to stagnation of oral secretions and drying of mucous membranes.
Collaborative
- Administer medications as indicated: Analgesics;
- Rationale: Reduce/control pain and decrease stimulation of the sympathetic nervous system.
- Antianxiety agents, e.g., lorazepam (ativan), alprazolam (xanax), diazepam (valium).
- Rationale: May aid in the reduction of tension and discomfort that is intensified by stress.
Nursing diagnosis: Imbalanced Nutrition (more than body requirements)
May be related to
- Excessive intake in relation to metabolic need
- Sedentary lifestyle
- Cultural preferences
Possibly evidenced by
- Weight 10%–20% more than ideal for height and frame
- Triceps skinfold more than 15 mm in men and 25 mm in women (maximum for age and sex)
- Reported or observed dysfunctional eating patterns
Desired outcomes/evaluation criteria—patient will:
- Identify correlation between hypertension and obesity.
- Demonstrate change in eating patterns (e.g., food choices, quantity) to attain desirable body weight with optimal maintenance of health.
- Initiate/maintain individually appropriate exercise program
Nursing Interventions
Weight reduction assistance
Independent
- Assess patient understanding of direct relationship between hypertension and obesity.
- Rationale: Obesity is an added risk with high blood pressure because of the disproportion between fixed aortic capacity andIncreased cardiac output associated with increased body mass. Reduction in weight may obviate the need for drug therapy or decrease the amount of medication needed for control of bp. Note: recent research suggests that bringing weight within 15% of ideal weight can result in a drop of 10 mm hg in both systolic and diastolic bp.
- Discuss necessity for decreased caloric intake and limited intake of fats, salt, and sugar as indicated.
- Rationale: Faulty eating habits contribute to atherosclerosis andObesity, which predispose to hypertension and subsequent complications, e.g., stroke, kidney disease, heart failure. Excessive salt intake expands the intravascular fluid volume and may damage kidneys, which can further aggravate hypertension. Note: one study showed that sodium reduction reduced the need for medication by 31%. Weight loss lowered the need for medication by 36% and the combination of the two by 53%.
- Determine patient’s desire to lose weight.
- Rationale: Motivation for weight reduction is internal. The individual must want to lose weight, or the program most likely will not succeed.
- Review usual daily caloric intake and dietary choices.
- Rationale: Identifies current strengths/weaknesses in dietary program. Aids in determining individual need for adjustment/teaching.
- Establish a realistic weight reduction plan with the patient, e.g., 1 lb weight loss/wk.
- Rationale: Reducing caloric intake by 500 calories daily theoretically yields a weight loss of 1 lb/wk. Slow reduction in weight is therefore indicative of fat loss with muscle sparing and generally reflects a change in eating habits.
- Encourage patient to maintain a diary of food intake, including when and where eating takes place and the circumstances and feelings around which the food was eaten.
- Rationale: Provides a database for both the adequacy of nutrients eaten and the emotional conditions of eating. Helps focus attention on factors that patient has control over/can change.
- Instruct and assist in appropriate food selections, such as a diet rich in fruits, vegetables, and low-fat dairy foods referred to as the dash dietary approaches to stop hypertension) diet and avoiding foods high in saturated fat (butter, cheese, eggs, ice cream, meat) and cholesterol (fatty meat, egg yolks, whole dairy products, shrimp, organ meats).
- Rationale: Avoiding foods high in saturated fat and cholesterol is important in preventing progressing atherogenesis. Moderation and use of low-fat products in place of total abstinence from certain food items may prevent sense of deprivation and enhance cooperation with dietary regimen. The dash diet, in conjunction with exercise, weight loss, and limits on salt intake, may reduce or even eliminate the need for drug therapy.
Collaborative
- Refer to dietitian as indicated.
- Rationale: Can provide additional counseling and assistance with meeting individual dietary needs.
Nursing diagnosis: Ineffective Coping
May be related to
- Situational/maturational crisis; multiple life changes
- Inadequate relaxation; little or no exercise, work overload
- Inadequate support systems
- Poor nutrition
- Unmet expectations; unrealistic perceptions
- Inadequate coping methods
Possibly evidenced by
- Verbalization of inability to cope or ask for help
- Inability to meet role expectations/basic needs or problem-solve
- Destructive behavior toward self; overeating, lack of appetite; excessive smoking/drinking, proneness to alcohol abuse
- Chronic fatigue/insomnia; muscular tension; frequent head/neck aches;
- Chronic worry, irritability, anxiety, emotional tension, depression
Desired outcomes/evaluation criteria—patient will:
Coping
- Identify ineffective coping behaviors and consequences.
- Verbalize awareness of own coping abilities/strengths.
- Identify potential stressful situations and steps to avoid/modify them.
- Demonstrate the use of effective coping skills/methods.
Nursing Interventions
Coping enhancement
Independent
- Assess effectiveness of coping strategies by observing behaviors, e.g., ability to verbalize feelings and concerns, willingness to participate in the treatment plan.
- Rationale: Adaptive mechanisms are necessary to appropriately alter one’s lifestyle, deal with the chronicity of hypertension, and integrate prescribed therapies into daily living.
- Note reports of sleep disturbances, increasing fatigue, impaired concentration, irritability, decreased tolerance of headache, inability to cope/problem-solve.
- Rationale: Manifestations of maladaptive coping mechanisms may be indicators of repressed anger and have been found to be major determinants of diastolic bp.
- Assist patient to identify specific stressors and possible strategies for coping with them.Include patient in planning of care, and encourage maximum participation in treatment plan.
- Rationale: Recognition of stressors is the first step in altering one’s response to the stressor.Involvement provides patient with an ongoing sense of control, improves coping skills, and can enhance cooperation with therapeutic regimen.
- Encourage patient to evaluate life priorities/goals. Ask questions such as “is what you are doing getting you what you want?”
- Rationale: Focuses patient’s attention on reality of present situation relative to patient’s view of what is wanted. Strong work ethic, need for “control,” and outward focus may have led to lack of attention to personal needs.
- Assist patient to identify and begin planning for necessary lifestyle changes. Assist to adjust, rather than abandon, personal/family goals.
- Rationale: Necessary changes should be realistically prioritized so patient can avoid being overwhelmed and feeling powerless.
Nursing diagnosis: Knowledge Deficit (learning need) regarding condition, treatment plan, self-care and discharge needs
May be related to
- Lack of knowledge/recall
- Information misinterpretation
- Cognitive limitation
- Denial of diagnosis
Possibly evidenced by
- Verbalization of the problem
- Request for information
- Statement of misconception
- Inaccurate follow-through of instructions; inadequate performance of procedures
- Inappropriate or exaggerated behaviors, e.g., hostile, agitated, apathetic
Desired outcomes/evaluation criteria—patient will:
- Verbalize understanding of disease process and treatment regimen.
- Identify drug side effects and possible complications that necessitate medical attention.
- Maintain bp within individually acceptable parameters.
Knowledge: treatment regimen
- Describe reasons for therapeutic actions/treatment regimen.
Nursing Interventions
Teaching: disease process
Independent
- Assess readiness and blocks to learning. Include significant other (so).
- Rationale: Misconceptions and denial of the diagnosis because of long-standing feelings of well-being may interfere with patient/so willingness to learn about disease, progression, and prognosis. If patient does not accept the reality of a life-threatening condition requiring continuing treatment, lifestyle/behavioral changes will not be initiated/sustained.
- Define and state the limits of desired bp. Explain hypertension and its effects on the heart, blood vessels, kidneys, and brain.
- Rationale: Provides basis for understanding elevations of bp, and clarifies frequently used medical terminology. Understanding that high bp can exist without symptoms is central to enabling patient to continue treatment, even when feeling well.
- Avoid saying “normal” bp, and use the term “well-controlled” to describe patient’s bp within desired limits.
- Rationale: Because treatment for hypertension is lifelong, conveying the idea of “control” helps patient understand the need for continued treatment/medication.
- Assist patient in identifying modifiable risk factors, e.g., obesity; diet high in sodium, saturated fats, and cholesterol; sedentary lifestyle; smoking; alcohol intake (more than 2 oz/day on a regular basis); stressful lifestyle.
- Rationale: These risk factors have been shown to contribute to hypertension and cardiovascular and renal disease.
- Problem-solve with patient to identify ways in which appropriate lifestyle changes can be made to reduce modifiable risk factors.
- Rationale: Changing “comfortable/usual” behavior patterns can be very difficult and stressful. Support, guidance, and empathy can enhance patient’s success in accomplishing these tasks.
- Discuss importance of eliminating smoking, and assist patient in formulating a plan to quit smoking.
- Rationale: Nicotine increases catecholamine discharge, resulting in increased heart rate, bp, vasoconstriction, and myocardial workload, and reduces tissue oxygenation.
- Reinforce the importance of adhering to treatment regimen and keeping follow-up appointments.
- Rationale: Lack of cooperation is a common reason for failure of antihypertensive therapy. Therefore, ongoing evaluation for patient cooperation is critical to successful treatment. Compliance usually improves when patient understands causative factors and consequences of inadequate intervention and health maintenance.
- Instruct and demonstrate technique of bp self-monitoring. Evaluate patient’s hearing, visual acuity, manual dexterity, and coordination.
- Rationale: Monitoring bp at home is reassuring to patient because it provides visual/positive reinforcement for efforts in following the medical regimen and promotes early detection of deleterious changes.
- Help patient develop a simple, convenient schedule for taking medications.
- Rationale: Individualizing medication schedule to fit patient’s personal habits/needs may facilitate cooperation with long-term regimen.
- Explain prescribed medications along with their rationale, dosage, expected and adverse side effects, and idiosyncrasies
- Rationale: Adequate information and understanding that side effects (e.g., mood changes, initial weight gain, dry mouth) are common and often subside with time can enhance cooperation with treatment plan.
- Diuretics: take daily doses (or larger dose) in the early morning;
- Rationale: Scheduling minimizes nighttime urination.
- Weigh self on a regular schedule and record
- Rationale: Primary indicator of effectiveness of diuretic therapy.
- Avoid/limit alcohol intake
- Rationale: The combined vasodilating effect of alcohol and the volume-depleting effect of a diuretic greatly increase the risk of orthostatic hypotension.
- Notify physician if unable to tolerate food or fluid
- Rationale: Dehydration can develop rapidly if intake is poor and patient continues to take a diuretic.
- Antihypertensives: take prescribed dose on a regular schedule; avoid skipping, altering, or making up doses; and do not discontinue without notifying the healthcare provider. Review potential side effects and/or drug interactions
- Rationale: Because patients often cannot feel the difference the medication is making in blood pressure, it is critical that there is understanding about the medications’ working and side effects. For example, abruptly discontinuing a drug may cause rebound hypertension leading to severe complications, or medication may need to be altered to reduce adverse effects.
- Rise slowly from a lying to standing position, sitting for a few minutes before standing. Sleep with the head slightly elevated.
- Rationale: Measures reduce severity of orthostatic hypotension associated with the use of vasodilators and diuretics.
- Suggest frequent position changes, leg exercises when lying down.
- Rationale: Decreases peripheral venous pooling that may be potentiated by vasodilators and prolonged sitting/standing.
- Recommend avoiding hot baths, steam rooms, and saunas, especially with concomitant use of alcoholic beverages.
- Rationale: Prevents vasodilation with potential for dangerous side effects of syncope and hypotension.
- Instruct patient to consult healthcare provider before taking other prescription or over-the-counter (otc) medications.
- Rationale: Precaution is important in preventing potentially dangerous drug interactions. Any drug that contains a sympathetic nervous stimulant may increase bp or counteract antihypertensive effects.
- Instruct patient about increasing intake of foods/fluids high in potassium, e.g., oranges, bananas, figs, dates, tomatoes, potatoes, raisins, apricots, gatorade, and fruit juices and foods/fluids high in calcium, e.g., low-fat milk, yogurt, or calcium supplements, as indicated.
- Rationale: Diuretics can deplete potassium levels. Dietary replacement is more palatable than drug supplements and may be all that is needed to correct deficit. Some studies show that 400 mg of calcium/day can lower systolic and diastolic bp. Correcting mineral deficiencies can also affect bp.
- Review signs/symptoms requiring notification of healthcare provider, e.g., headache present on awakening that does not abate; sudden and continued increase of bp; chest pain/shortness of breath; irregular/increased pulse rate; significant weight gain (2 lb/day or 5 lb/wk) or peripheral/abdominal swelling; visual disturbances; frequent, uncontrollable nosebleeds; depression/emotional lability; severe dizziness or episodes of fainting; muscle weakness/cramping; nausea/vomiting; excessive thirst.
- Rationale: Early detection of developing complications/decreased effectiveness of drug regimen or adverse reactions to it allows for timely intervention.
- Explain rationale for prescribed dietary regimen (usually a diet low in sodium, saturated fat, and cholesterol).
- Rationale: Excess saturated fats, cholesterol, sodium, alcohol, and calories have been defined as nutritional risks in hypertension. A diet low in fat and high in polyunsaturated fat reduces bp, possibly through prostaglandin balance in both normotensive and hypertensive people.
- Help patient identify sources of sodium intake (e.g., table salt, salty snacks, processed meats and cheeses, sauerkraut, sauces, canned soups and vegetables, baking soda, baking powder, monosodium glutamate). Stress the importance of reading ingredient labels of foods and otc drugs.
- Rationale: Two years on a moderate low-salt diet may be sufficient to control mild hypertension or reduce the amount of medication required.
- Encourage patient to establish an individual exercise program incorporating aerobic exercise (walking, swimming) within patient’s capabilities. Stress the importance of avoiding isometric activity.
- Rationale: Besides helping to lower bp, aerobic activity aids in toning the cardiovascular system. Isometric exercise can increase serum catecholamine levels, further elevating bp.
- Demonstrate application of ice pack to the back of the neck and pressure over the distal third of nose, and recommend that patient lean the head forward, if nosebleed occurs.
- Rationale: Nasal capillaries may rupture as a result of excessive vascular pressure. Cold and pressure constrict capillaries to slow or halt bleeding. Leaning forward reduces the amount of blood that is swallowed.
- Provide information regarding community resources, and support patient in making lifestyle changes. Initiate referrals as indicated.
- Rationale: Community resources such as the american heart association, “coronary clubs,” stop smoking clinics, alcohol (drug) rehabilitation, weight loss programs, stress management classes, and counseling services may be helpful in patient’s efforts to initiate and maintain lifestyle changes.


