Notes
Description
- Congestive Heart Failure or CHF is a severe circulatory congestion due to decreased myocardial contractility, which results in the heart’s inability to pump sufficient blood to meet the body’s needs.

- About 80% of CHF cases occur before 1 year of age
Etiology
- The primary cause of CHF in the first 3 years of life is CHD.
- Other causes in children include:
- Other myocardial disorders, such as cardiomyopathies, arrhythmias, and hypertension
- Pulmonary embolism or chronic lung disease
- Severe hemorrhage or anemia
- Adverse effects of anesthesia or surgery
- Adverse effects of transfusions or infusions
- Increased body demands resulting from conditions such as fever, infection and arteriovenous fistula
- Adverse effects of drugs, such as doxorubicin
- Severe physical or emotional stress
- Excessive sodium intake
- In general, causes can be classified according to the following:
- Volume overload may cause the right ventricle to hypertrophy to compensate for added volume.
- Pressure overload usually results from an obstructive lesion, such as COA
- Decrease contractility can result from problems such as sever anemia, asphyxia, heart block and acidemia.
- High cardiac output demands occur when the body’s need for oxygen exceeds the heart’s output s seen in sepsis and hyperthyroidism.
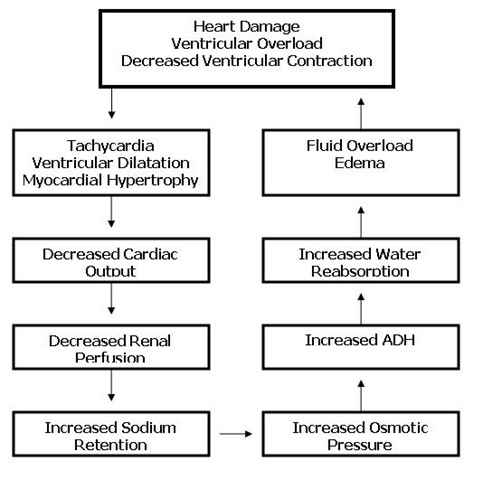
Pathophysiology
- Right ventricular failure occurs when the right ventricle is unable to pump blood into the pulmonary circulation. Less blood is oxygenated and pressure increases in the right atrium and systemic venous circulation, which results in edema of the extremities.
- Left ventricular failure occurs when the left ventricle in unable to pump blood into systemic circulation. Pressure increases in the left atrium and pulmonary veins; then the lungs become congested with blood, causing elevated pulmonary pressure and pulmonary edema.
- To compensate, the cardiac muscle hypertrophies eventually resulting in decreased ventricular compliance. Decreased compliance requires higher filling pressure to produce the same stroke volume. Increased muscle mass impedes oxygenation of the heart muscle, which leads to decreased contraction force and heart failure.
- As cardiac output fails, stretch receptors and baroreceptors stimulate the sympathetic nervous system, releasing catecholamines that increase the force and rate of myocardial contraction.
- This causes increased systemic resistance, increased venous return, and reduced blood flow to the limbs, viscera and kidneys.
- Sweating results from sympathetic cholinergic fibers, there is extra work for the heart muscle, and there is less systemic blood flow.
- The renal system responds by releasing renin-angiotensin, which sets off a chain of events – vasoconstriction, leading to increased aldosterone release, causing sodium and water retention and, in turn, increasing preload. Finally, sodium and water retention becomes excessive, resulting in signs of systemic venous congestion and fluid overload.
Assessment
- Right ventricular failure
- Signs of right ventricular failure are evident in the systemic circulation
- Pitting, dependent edema in the feet, legs, sacrum, back, and buttocks
- Ascites from portal hypertension
- Tenderness of right upper quadrant, organomegaly
- Distended neck veins
- Pulsus alternans (regular alteration of weak and strong beats noted in the pulse)
- Abdominal pain, bloating
- Anorexia, nausea
- Fatigue
- Weight gain
- Nocturnal diuresis
- Left ventricular failure
- Signs of left ventricular failure are evident in the pulmonary system
- Cough, which may become productive with frothy sputum
- Dyspnea on exertion
- Orthopnea
- Paroxysmal nocturnal dyspnea
- Presence of crackles on auscultation
- Tachycardia
- Pulsus alternans
- Fatigue
- Pallor
- Cyanosis
- Confusion and disorientation
- Signs of cerebral anoxia
- Acute pulmonary edema
- Severe dyspnea and orthopnea
- Pallor
- Tachycardia
- Expectoration of large amounts of blood-tinged, frothy sputum
- Wheezing and crackles on auscultation
- Bubbling respirations
- Acute anxiety, apprehension, restlessness
- Profuse sweating
- Cold, clammy skin
- Cyanosis
- Nasal flaring
- Use of accessory breathing muscles
- Tachypnea
- Hypocapnia, evidenced by muscle cramps, weakness, dizziness, and paresthesias
Diagnostic Evaluation
- Chest radiography reveals cardiomegaly and pulmonary congestion
- CBC reveals dilution hyponatremia, hypochloremia, and hyperkalemia
- ECG reveals ventricular hypertrophy
Primary Nursing Diagnosis
- Decreased CO related to an ineffective ventricular pump
Medical Management
- Initial management of the patient with HF depends on severity of HF, seriousness of symptoms, etiology, presence of other illnesses, and precipitating factors. Medication management is paramount in patients with HF. The general principles for management are treatment of any precipitating causes, control of fluid and sodium retention, increasing myocardial contractility, decreasing cardiac workload, and reducing pulmonary and systemic venous congestion. The physician may also prescribe fluid and sodium restriction in an attempt to reduce volume and thereby reduce preload.
Surgical Management
- Coronary bypass surgery, PTCA, other innovative therapies as indicated (e.g, mechanical assist devices , transplantation)
Pharmacologic Intervention
Alone or in combination: vasodilator therapy (angiotensin-converting enzyme (ACE) inhibitors), angiotensin II receptor blockers (ARBs), select beta-blockers, calcium channel blockers, diuretic therapy, cardiac glycosides (digitalis), and others
- Dobutamine, milrinone, anticoagulants, beta-blockers, as indicated
- Possibly antihypertensives or antianginal medications and anticoagulants
Nursing Intervention
- Monitor for signs of respiratory distress
- Provide pulmonary hygiene as needed
- Administer oxygen as prescribed
- Keep the head of the bed elevated
- Monitor ABG values.
- Monitor for signs of altered cardiac output, including
- Pulmonary edema
- Arrhythmias, including extreme tachycardia and bradycardia
- Characteristic ECG and heart sound changes
- Evaluate fluid status
- Maintain strict fluid intake and output measurements
- Monitor daily weights
- Assess for edema and severe diaphoresis
- Monitor electrolyte values and hematocrit level
- Maintain strict fluid restrictions as prescribed
- Administer prescribed medications which may include:
- Antiarrhythmias to increase cardiac performance
- Diuretics, to reduce venous and systemic congestion
- Iron and folic acid supplements to improve nutritional status.
- Prevent Infection
- Reduce cardiac demands
- Keep the child warm
- Schedule nursing interventions to allow for rest
- Do not allow an infant to feed for more than 45 minutes at a time
- Provide gavage feedings if the infant becomes fatigued before ingesting an adequate amount
- Promote adequate nutrition. Maintain a high-calorie, low-sodium as prescribed.
- Promote optimal growth and development
- As appropriate, refer the family to a community health nurse for follow up care after discharge.
Documentation Guidelines
- Physical findings indicative of HF:Mental confusion,pale,cyanotic,clammy skin,presence of jugular vein distension and HJR,ascites,edema,pulmonary crackles or wheezes,adventitious heart sounds
- Fluid intake and output,daily weights
- Response to medications such as diuretics,nitrates,dopamine,dobutamine,and oxygen
- Psychosocial response to illness
Discharge and Home Healthcare Guidelines
- PREVENTION. To prevent exacerbations, teach the patient and family to monitor for an increase in shortness of breath or edema. Tell the patient to restrict fluid intake to 2 to 2.5 L per day and restrict sodium intake as prescribed. Teach the patient to monitor daily weights and report weight gain of more than 4 pounds in 2 days.
- MEDICATIONS. Be sure the patient and family understand all medications, including effect, dosage, route, adverse effects, and the need for routine laboratory monitoring for drugs such as digoxin.
- COMPLICATIONS OF HF. Tell the patient to call for emergency assistance for acute shortness of breath or chest discomfort that is not alleviated with rest.
Sources:
Marilyn Sawyer Sommers, RN, PhD, FAAN , Susan A. Johnson, RN, PhD, Theresa A. Beery, PhD, RN , DISEASES AND DISORDERS A Nursing Therapeutics Manual, 2007 3rd ed
Lippincott’s Review Series – Pediatric Nursing
Handbook for Brunner & Suddarth’s ,Textbook of Medical-Surgical Nursing, 11th ed
Exam
Nursing Care Plan
Decreased Cardiac Output
Assessment
The patient may manifest the following:
- Pale conjunctiva, nail beds, and buccal mucosa
- irregular rhythm of pulse
- bradycardia
- generalized weakness
Diagnosis
- Decreased cardiac output r/t [altered heart rate and rhythm] AEB [bradycardia]
Planning
- Short Term: After 3-4 hours of nursing interventions, the patient will participate in activities that reduce the workload of the heart.
- Long Term: After 2-3 days of nursing interventions, the patient will be able to display hemodynamic stability.
Nursing Interventions
- Assess for abnormal heart and lung sounds.
- Rationale: Allows detection of left-sided heart failure that may occur with chronic renal failure patients due to fluid volume excess as the diseased kidneys are unable to excrete water.
- Monitor blood pressure and pulse.
- Rationale: Patients with renal failure are most often hypertensive, which is attributable to excess fluid and the initiation of the rennin-angiotensin mechanism.
- Assess mental status and level of consciousness.
- Rationale: The accumulation of waste products in the bloodstream impairs oxygen transport and intake by cerebral tissues, which may manifest itself as confusion, lethargy, and altered consciousness.
- Assess patient’s skin temperature and peripheral pulses.
- Rationale: Decreased perfusion and oxygenation of tissues secondary to anemia and pump ineffectiveness may lead to decreased in temperature and peripheral pulses that are diminished and difficult to palpate.
- Monitor results of laboratory and diagnostic tests.
- Rationale: Results of the test provide clues to the status of the disease and response to treatments.
- Monitor oxygen saturation and ABGs.
- Rationale: Provides information regarding the heart’s ability to perfuse distal tissues with oxygenated blood
- Give oxygen as indicated by patient symptoms, oxygen saturation and ABGs.
- Rationale: Makes more oxygen available for gas exchange, assisting to alleviate signs of hypoxia and subsequent activity intolerance.
- Implement strategies to treat fluid and electrolyte imbalances.
- Rationale: Decreases the risk for development of cardiac output due to imbalances.
- Administer cardiac glycoside agents, as ordered, for signs of left sided failure, and monitor for toxicity.
- Rationale: Digitalis has a positive isotropic effect on the myocardium that strengthens contractility, thus improving cardiac output.
- Encourage periods of rest and assist with all activities.
- Rationale: Reduces cardiac workload and minimizes myocardial oxygen consumption.
- Assist the patient in assuming a high Fowler’s position.
- Rationale: Allows for better chest expansion, thereby improving pulmonary capacity.
- Teach patient the pathophysiology of disease, medications
- Rationale: Provides the patient with needed information for management of disease and for compliance.
- Reposition patient every 2 hours
- Rationale: To prevent occurrence of bed sores
- Instruct patient to get adequate bed rest and sleep
- Rationale: To promote relaxation to the body
- Instruct the SO not to leave the client unattended
- Rationale: To ensure safety and reduce risk for falls that may lead to injury
Evaluation
- After nursing interventions, the patient shall have participated in activities that reduce the workload of the heart.
- After 2-3 days of nursing interventions, the patient shall have been able to display hemodynamic stability.
Excess Fluid Volume
Assessment
The patient may manifest the following:
- Edema of extremities
- Difficulty of breathing
- Crackles
- Change in mental status
- Restlessness and anxiety
Diagnosis
- Excessive Fluid volume related to decreased cardiac output and sodium and water retention
Planning & Desired Outcomes
- Patient will verbalize understanding of causative factors and demonstrate behaviors to resolve excess fluid volume.
- Patient will demonstrate adequate fluid balanced AEB output equal to exceeding intake, clearing breath sounds, and decreasing edema.
Nursing Interventions
- Establish rapport
- Rationale: To gain patient’s trust and cooperation
- Monitor and record VS
- Rationale: To obtain baseline data
- Assess patient’s general condition
- Rationale: To determine what approach to use in treatment
- Monitor I&O every 4 hours
- Rationale: I&O balance reflects fluid status
- Weigh patient daily and compare to previous weights.
- Rationale: Body weight is a sensitive indicator of fluid balance and an increase indicates fluid volume excess.
- Auscultate breath sounds q 2hr and pm for the presence of crackles and monitor for frothy sputum production
- Rationale: When increased pulmonary capillary hydrostatic pressure exceeds oncotic pressure, fluid moves within the alveolar septum and is evidenced by the auscultation of crackles. Frothy, pink-tinged sputum is an indicator that the client is developing pulmonary edema
- Assess for presence of peripheral edema. Do not elevate legs if the client is dyspneic.
- Rationale: Decreased systemic blood pressure to stimulation of aldosterone, which causes increased renal tubular absorption of sodium Low-sodium diet helps prevent increased sodium retention, which decreases water retention. Fluid restriction may be used to decrease fluid intake, hence decreasing fluid volume excess.
- Follow low-sodium diet and/or fluid restriction
- Rationale: The client senses thirst because the body senses dehydration. Oral care can alleviate the sensation without an increase in fluid intake.
- Encourage or provide oral care q2
- Rationale: Heart failure causes venous congestion, resulting in increased capillary pressure. When hydrostatis pressure exceeds interstitial pressure, fluids leak out of ht ecpaillaries and present as edema in the legs, and sacrum. Elevation of legs increases venous return to the heart.
- Obtain patient history to ascertain the probable cause of the fluid disturbance.
- Rationale: May include increased fluids or sodium intake, or compromised regulatory mechanisms.
- Monitor for distended neck veins and ascites
- Rationale: Indicates fluid overload
- Evaluate urine output in response to diuretic therapy.
- Rationale: Focus is on monitoring the response to the diuretics, rather than the actual amount voided
- Assess the need for an indwelling urinary catheter.
- Rationale: Treatment focuses on diuresis of excess fluid.
- Institute/instruct patient regarding fluid restrictions as appropriate.
- Rationale: This helps reduce extracellular volume.
Acute Pain
Assessment
Patient may manifest the following
- Difficulty of breathing
- Chest pain
- Restlessness
Diagnosis
- Acute Pain
Planning & Desired Outcomes
- Patient’s pain will be decreased.
- Patient will demonstrate activities and behaviors that will prevent the recurrence of pain.
Nursing Interventions
- Assess patient pain for intensity using a pain rating scale, for location and for precipitating factors.
- Rationale: To identify intensity, precipitating factors and location to assist in accurate diagnosis.
- Administer or assist with self-administration of vasodilators, as ordered.
- Rationale: The vasodilator nitroglycerin enhances blood flow to the myocardium. It reduces the amount of blood returning to the heart, decreasing preload which in turn decreases the workload of the heart.
- Assess the response to medications every 5 minutes
- Rationale: Assessing response determines effectiveness of medication and whether further interventions are required.
- Provide comfort measures.
- Rationale: To provide nonpharmacological pain management.
- Establish a quiet environment.
- Rationale: A quiet environment reduces the energy demands on the patient.
- Elevate head of bed.
- Rationale: Elevation improves chest expansion and oxygenation.
- Monitor vital signs, especially pulse and blood pressure, every 5 minutes until pain subsides.
- Rationale: Tachycardia and elevated blood pressure usually occur with angina and reflect compensatory mechanisms secondary to sympathetic nervous system stimulation.
- Teach patient relaxation techniques and how to use them to reduce stress.
- Rationale: Anginal pain is often precipitated by emotional stress that can be relieved non-pharmacological measures such as relaxation.
- Teach the patient how to distinguish between angina pain and signs and symptoms of myocardial infarction.
- Rationale: In some case, the chest pain may be more serious than stable angina. The patient needs to understand the differences in order to seek emergency care in a timely fashion.
Ineffective Tissue Perfusion
Assessment
- Pale conjunctiva, nail beds, and buccal mucosa
- Generalized weakness
- Chest pain
- Difficulty of breathing
- Abnormal pulse rate and rhythm
- Bradycardia
- Altered BP readings
- With pitting edema on both forearms and hands
- Bipedal pitting edema
Diagnosis
- Ineffective tissue perfusion related to decreased cardiac output.
Planning & Desired Outcomes
- Patient will demonstrate behaviors to improve circulation.
- Display vital signs within acceptable limits, dysrhythmias absent/controlled,and no symptoms of failure
Nursing Interventions
- Assess patient pain for intensity using a pain rating scale, for location and for precipitating factors.
- Rationale: To identify intensity, precipitating factors and location to assist in accurate diagnosis.
- Administer or assist with self administration of vasodilators, as ordered.
- Rationale: The vasodilator nitroglycerin enhances blood flow to the myocardium. It reduces the amount of blood returning to the heart, decreasing preload which in turn decreases the workload of the heart.
- Assess the response to medications every 5 minutes.
- Rationale: Assessing response determines effectiveness of medication and whether further interventions are required.
- Give beta blockers as ordered.
- Rationale: Beta blockers decrease oxygen consumption by the myocardium and are given to prevent subsequent angina episodes.
- Establish a quiet environment.
- Rationale: A quiet environment reduces the energy demands on the patient.
- Elevate head of bed.
- Rationale: Elevation improves chest expansion and oxygenation.
- Monitor vital signs, especially pulse and blood pressure, every 5 minutes until pain subsides.
- Rationale: Tachycardia and elevated blood pressure usually occur with angina and reflect compensatory mechanisms secondary to sympathetic nervous system stimulation.
- Provide oxygen and monitor oxygen saturation via pulse oximetry, as ordered.
- Rationale: Oxygenation increases the amount of oxygen circulating in the blood and, therefore, increases the amount of available oxygen to the myocardium, decreasing myocardial ischemia and pain.
- Assess results of cardiac markers—creatinine phosphokinase, CK- MB, total LDH, LDH-1, LDH-2, troponin, and myoglobin ordered by physician.
- Rationale: These enzymes elevate in the presence of myocardial infarction at differing times and assist in ruling out a myocardial infarction as the cause of chest pain.
- Assess cardiac and circulatory status.
- Rationale: Assessment establishes a baseline and detects changes that may indicate a change in cardiac output or perfusion.
- Monitor cardiac rhythms on patient monitor and results of 12 lead ECG.
- Rationale: Notes abnormal tracings that would indicate ischemia.
- Teach patient relaxation techniques and how to use them to reduce stress.
- Rationale: Anginal pain is often precipitated by emotional stress that can be relieved non-pharmacological measures such as relaxation.
- Teach the patient how to distinguish between angina pain and signs and symptoms of myocardial infarction.
- Rationale: In some case, the chest pain may be more serious than stable angina. The patient needs to understand the differences in order to seek emergency care in a timely fashion.
- Reposition the patient every 2 hours
- Rationale: To prevent bedsores
- Instruct patient on eating a small frequent feedings
- Rationale: To prevent heartburn and acid indigestion
Hyperthermia
Assessment
Patient may manifest the following:
- Pale palpebral
- Conjunctiva and nail beds
- Warm to touch
- Weakness
- Increased in body temperature
- Fluid or electrolyte imbalance
- Diaphoresis
- Hot flushed skin
Diagnosis
- Hyperthermia RT increased metabolic rate secondary to pneumonia
Planning & Desired Outcomes
- Patient’s temperature will be on normal level.
Nursing Interventions
- Assess vital signs, the temperature.
- Rationale: Vital signs provide more accurate indication.
- Monitor and record all sources of fluid loss such as urine, vomiting and diarrhea.
- Rationale: For potential fluid and electrolyte losses.
- Performed tepid sponge bath.
- Rationale: To promote heat loss by evaporation and conduction.
- Maintain bed rest.
- Rationale: To reduce metabolic demands and oxygen consumption.
- Remove excess clothing and covers.
- Rationale: Decreases warmth and increase evaporative cooling.
- Increase fluid intake.
- Rationale: To prevent dehydration.
- Provide adequate nutrition, a high caloric diet.
- Rationale: The meet the metabolic demands.
- Control environmental temperature.
- Rationale: To prevent an increase in body temperature and prevent shivering of the patient.
- Adjust cooling measures on the basis of physical response.
- Rationale: Shivering, which burns calories and increases metabolic rate in order to produce heat.
- Provide information regarding normal temperature and control.
- Rationale: This is especially necessary for patients with conditions at risk for hyperthermia.
- Explain all treatments.
- Rationale: Patients’ S.O. needs to be oriented.
- Administer antipyretics as ordered.
- Rationale: To decrease body temperature.
- Control excessive shivering with medications such as Chlorpromazine and Diazepam if necessary.
- Rationale: Shivering increases metabolic rate and body temperature.
- Provide ample fluids by mouth or intravenously as ordered.
- Rationale: If the patient is dehydrated or diaphoretic, fluid loss contributes to fever.
- Provide oxygen therapy in extreme cases as ordered.
- Rationale: Hyperthermia increases metabolism.
Ineffective Breathing Pattern
Assessment
Patient may manifest the following:
- weakness
- rales on BLF
- productive cough
- frothy sputum
- pursed lip breathing
- tachypnea
Diagnosis
- Ineffective breathing pattern related to fatigue and decreased lung expansion and pulmonary congestion secondary to CHF
Planning & Desired Outcomes
- Patient’s respiratory pattern will be effective without causing fatigue
Nursing Interventions
- Establish rapport
- Rationale: To gain comfort feelings form the pt and pts SO
- Monitor VS
- Rationale: To gain baseline data
- Inspect thorax for symmetry of respiratory movement
- Rationale: Determines adequacy of breathing
- Observe breathing pattern for SOB, nasal flaring, pursed-lip breathing or prolonged expiratory phase and use of accessory muscles
- Rationale: Identifies increased work of breathing
- Measure tidal volume and vital capacity
- Rationale: Indicates volume of air moving in and out of lungs
- Assess emotional response
- Rationale: Detects use of hyperventilation as a causative factor
- Position patient in optimal body alignment in semi- fowler’s position for breathing
- Assist patient to use relaxation techniques
- Rationale: Reduces muscle tension, decreases work of breathing
Activity Intolerance
Assessment
- Weakness
- Limited range of motion
- Abnormal pulse rate and rhythm
Diagnosis
- Activity intolerance r/t imbalance O2 supply and demand
Planning & Desired Outcomes
- Patient will use identified techniques to improve activity intolerance
- Patient will report measurable increase in activity intolerance
Nursing Interventions
- Establish Rapport
- Rationale: To gain clients participation and cooperation in the nurse patient interaction
- Monitor and record Vital Signs
- Rationale: To obtain baseline data
- Assess patient’s general condition
- Rationale: To note for any abnormalities and deformities present within the body
- Adjust client’s daily activities and reduce intensity of level. Discontinue activities that cause undesired psychological changes
- Rationale: To prevent strain and overexertion
- Instruct client in unfamiliar activities and in alternate ways of conserve energy
- Rationale: To conserve energy and promote safety
- Encourage patient to have adequate bed rest and sleep
- Rationale: to relax the body
- Provide the patient with a calm and quiet environment
- Rationale: to provide relaxation
- Assist the client in ambulation
- Rationale: to prevent risk for falls that could lead to injury
- Note presence of factors that could contribute to fatigue
- Rationale: fatigue affects both the client’s actual and perceived ability to participate in activities
- Ascertain client’s ability to stand and move about and degree of assistance needed or use of equipment
- Rationale: to determine current status and needs associated with participation in needed or desired activities
- Give client information that provides evidence of daily or weekly progress
- Rationale: to sustain motivation of client
- Encourage the client to maintain a positive attitude
- Rationale: to enhance sense of well being
- Assist the client in a semi-fowlers position
- Rationale: to promote easy breathing
- Elevate the head of the bed
- Rationale: to maintain an open airway
- Assist the client in learning and demonstrating appropriate safety measures
- Rationale: to prevent injuries
- Instruct the SO not to leave the client unattended
- Rationale: to avoid risk for falls
- Provide client with a positive atmosphere
- Rationale: to help minimize frustration and rechannel energy
- Instruct the SO to monitor response of patient to an activity and recognize the signs and symptoms
- Rationale: to indicate need to alter activity level