Notes
Definition of Colostomy
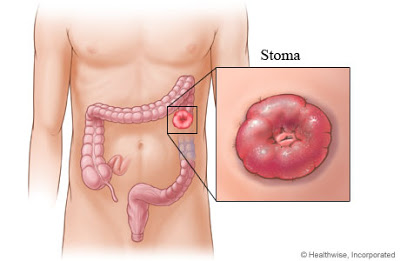
- Colostomy is a surgical procedure that brought formation of an opening into the colon, brought out onto the abdominal wall as a stoma. The opening can be either permanent or temporary.
Specific Technique for Colostomy
- Bowel technique
Discussion
- This procedure is usually performed for lesions in the large intestine caused by cancer, diverticulitis, or obstruction of the large intestine in an area close to the rectum.
- Types of colostomy:
- Temporary colostomy: A temporary colostomy is performed to divert the fecal stream from the distal colon, which may be obstructed by tumor inflammation, or requires being “put-to-test” because of anastomosis or a pouch procedure. A temporary colostomy may be created in the transverse colon or sigmoid colon.
- Permanent colostomy: A permanent colostomy is performed to treat malignancies of the colon. Other indications may include irrevocable rectal strictures, incontinence of bowel, or inflammatory bowel disease. A permanent colostomy can be fashioned similar to a temporary colostomy but most often is an end colostomy.
Position
- Supine, with arms extended on arm boards.
Incision Site
- Dependent on the segment of colon to be used.
Packs/ Drapes
- Laparotomy pack

- Four folded towels
- Transverse Lap sheet
- Minor pack
Instrumentation
- Major Lap tray
- Intestinal tray
- Closing tray
- Internal surgical staples
Supplies/ Equipments
- Basin set
- Blades
- Needle counter
- Penrose drain
- Internal stapling instruments
- Glass rod and tubing with colostomy pouch
- Solutions – saline, water
- Sutures
- Medications
- Dressings
Procedure
- The abdomen is opened in the usual manner and the segment of colon is mobilized.
- The colon can be brought out through the main incision, or through an adjacent site from which a disk of skin and subcutaneous tissue has been excised.
- The underlying rectus fascia muscle and peritoneal layers are incised to accommodate the colon. The appropriate segment is excised between two atraumatic (intestinal) clamps or the internal stapling instrument, which is used to prepare and create the stoma.
- In a loop colostomy, a rod or bridge may be placed under the colon to avoid retraction.
- The abdomen is irrigated with warm saline and closed layers in a routine fashion.
- A colostomy poucj is applied over the stoma.
Perioperative Nursing Considerations
- The colostomy pouch may or may not be applied in surgery.
- A Vaseline gauze may encircle the stoma with a “fluff” type dressing applied.
- If the institution has an “Ostomy Nurse”, the application of the colostomy pouch may be delayed until the clinical specialist can work with the patient and family.
Exam
Nursing Care Plan
Nursing Diagnosis
- Fluid Volume, risk for deficient
Risk factors may include
- Excessive losses through normal routes, e.g., preoperative emesis and diarrhea; high-volume ileostomy output
- Losses through abnormal routes, e.g., NG/intestinal tube, perineal wound drainage tubes
- Medically restricted intake
- Altered absorption of fluid, e.g., loss of colon function
- Hypermetabolic states, e.g., inflammation, healing process
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired Outcomes
- Maintain adequate hydration as evidenced by moist mucous membranes, good skin turgor and capillary refill, stable vital signs, and individually appropriate urinary output.
Nursing Interventions
- Monitor intake and output (I&O) carefully, measure liquid stool. Weigh regularly.
- Rationale: Provides direct indicators of fluid balance. Greatest fluid losses occur with ileostomy, but they generally do not exceed 500–800 mL/day.
- Monitor vital signs, noting postural hypotension, tachycardia. Evaluate skin turgor, capillary refill, and mucous membranes.
- Rationale: Reflects hydration status and/or possible need for increased fluid replacement.
- Limit intake of ice chips during period of gastric intubation.
- Rationale: Ice chips can stimulate gastric secretions and wash out electrolytes.
- Monitor laboratory results, e.g., Hct and electrolytes
- Rationale: Detects homeostasis or imbalance, and aids in determining replacement needs
- Administer IV fluid and electrolytes as indicated.
- Rationale: May be necessary to maintain adequate tissue perfusion/organ function.
Nursing Diagnosis
- Skin/Tissue Integrity, impaired
May be related to
- Invasion of body structure (e.g., perineal resection)
- Stasis of secretions/drainage
- Altered circulation, edema; malnutrition
Possibly evidenced by
- Disruption of skin/tissue: presence of incision and sutures, drains
Desired Outcomes
- Achieve timely wound healing free of signs of infection.
Nursing Interventions
- Observe wounds, note characteristics of drainage.
- Rationale:Postoperative hemorrhage is most likely to occur during first 48 hr, whereas infection may develop at any time. Depending on type of wound closure (e.g., first or second intention), complete healing may take 6-8 mo.
- Change dressings as needed using aseptic technique
- Rationale: Large amounts of serous drainage require that dressings be changed frequently to reduce skin irritation and potential for infection.
- Encourage side-lying position with head elevated. Avoid prolonged sitting.
- Rationale: Promotes drainage from perineal wound/drains, reducing risk of pooling. Prolonged sitting increases perineal pressure, reducing circulation to wound, and may delay healing.
- Irrigate wound as indicated, using normal saline (NS), diluted hydrogen peroxide, or antibiotic solution.
- Rationale: May be required to treat preoperative inflammation and/or infection or intraoperative contamination.
- Provide sitz baths.
- Rationale: Promotes cleanliness and facilitates healing, especially after packing is removed (usually day 3–5).
Nursing Diagnosis
- Acute Pain
May be related to
- Physical factors: e.g., disruption of skin/tissues (incisions/drains)
- Biological: activity of disease process (cancer, trauma)
- Psychological factors: e.g., fear, anxiety
Possibly evidenced by
- Reports of pain, self-focusing
- Guarding/distraction behaviors, restlessness
- Autonomic responses, e.g., changes in vital signs
Desired Outcomes
- Verbalize that pain is relieved/controlled.
- Display relief of pain, able to sleep/rest appropriately
- Demonstrate use of relaxation skills and general comfort measures as indicated for individual situation.
Nursing Interventions
- Assess pain, noting location, characteristics, intensity (0–10 scale).
- Rationale: Helps evaluate degree of discomfort and effectiveness of analgesia or may reveal developing complications. Because abdominal pain usually subsides gradually by the third or fourth postoperative day, continued or increasing pain may reflect delayed healing or peristomal skin irritation. Note: Pain in anal area associated with abdominal-perineal resection may persist for months.
- Encourage patient to verbalize concerns. Active-listen these concerns, and provide support by acceptance, remaining with patient, and giving appropriate information.
- Rationale: Reduction of anxiety/fear can promote relaxation or comfort.
- Provide comfort measures, e.g., mouth care, back rub, repositioning (use proper support measures as needed). Assure patient that position change will not injure stoma.
- Rationale: Prevents drying of oral mucosa and associated discomfort. Reduces muscle tension, promotes relaxation, and may enhance coping abilities.
- Encourage use of relaxation techniques, e.g., guided imagery, visualization. Provide diversional activities.
- Rationale: Helps patient rest more effectively and refocuses attention, thereby reducing pain and discomfort.
- Assist with ROM exercises and encourage early ambulation. Avoid prolonged sitting position.
- Rationale: Reduces muscle/joint stiffness. Ambulation returns organs to normal position and promotes return of usual level of functioning. Note: Presence of edema, packing, and drains (if perineal resection has been done) increases discomfort and creates a sense of needing to defecate. Ambulation and frequent position changes reduce perineal pressure.
- Investigate and report abdominal muscle rigidity, involuntary guarding, and rebound tenderness.
- Rationale: Suggestive of peritoneal inflammation, which requires prompt medical intervention.
- Administer medication as indicated, e.g., narcotics, analgesics, patient-controlled analgesia (PCA).
- Rationale: Relieves pain, enhances comfort, and promotes rest. PCA may be more beneficial, especially following anal-perineal repair.
- Provide sitz baths.
- Rationale: Relieves local discomfort, reduces edema, and promotes healing of perineal wound.
- Apply/monitor effects of transcutaneous electrical nerve stimulator (TENS) unit.
- Rationale: Cutaneous stimulation may be used to block transmission of pain stimulus.
Nursing Diagnosis
- Body Image, disturbed
May be related to
- Biophysical: presence of stoma; loss of control of bowel elimination
- Psychosocial: altered body structure
- Disease process and associated treatment regimen, e.g., cancer, colitis
Possibly evidenced by
- Verbalization of change in body image, fear of rejection/reaction of others, and negative feelings about body
- Actual change in structure and/or function (ostomy)
- Not touching/looking at stoma, refusal to participate in care
Desired Outcomes
- Verbalize acceptance of self in situation, incorporating change into self-concept without negating self-esteem.
- Demonstrate beginning acceptance by viewing/touching stoma and participating in self-care.
- Verbalize feelings about stoma/illness; begin to deal constructively with situation.
Nursing Interventions
- Ascertain whether support and counseling were initiated when the possibility and/or necessity of ostomy was first discussed.
- Rationale: Provides information about patient’s/SO’s level of knowledge and anxiety about individual situation.
- Encourage patient/SO to verbalize feelings regarding the ostomy. Acknowledge normality of feelings of anger, depression, and grief over loss. Discuss daily “ups and downs” that can occur.
- Rationale: Helps patient realize that feelings are not unusual and that feeling guilty about them is not necessary or helpful. Patient needs to recognize feelings before they can be dealt with effectively.
- Review reason for surgery and future expectations.
- Rationale: Patient may find it easier to accept or deal with an ostomy done to correct chronic or long-term disease than for traumatic injury, even if ostomy is only temporary. Also, patient who will be undergoing a second procedure (to convert ostomy to a continent or anal reservoir) may possibly encounter less severe self-image problems because body function eventually will be “more normal.”
- Note behaviors of withdrawal, increased dependency, manipulation, or non involvement in care.
- Rationale: Suggestive of problems in adjustment that may require further evaluation and more extensive therapy.
- Provide opportunities for patient/SO to view and touch stoma, using the moment to point out positive signs of healing, normal appearance, and so forth. Remind patient that it will take time to adjust, both physically and emotionally.
- Rationale: Although integration of stoma into body image can take months or even years, looking at the stoma and hearing comments (made in a normal, matter-of-fact manner) can help patient with this acceptance. Touching stoma reassures patient/SO that it is not fragile and that slight movements of stoma actually reflect normal peristalsis.
- Provide opportunity for patient to deal with ostomy through participation in self-care.
- Rationale: Independence in self-care helps improve self-confidence and acceptance of situation.
- Plan/schedule care activities with patient.
- Rationale: Promotes sense of control and gives message that patient can handle situation, enhancing self-concept.
- Maintain positive approach during care activities, avoiding expressions of disdain or revulsion. Do not take angry expressions of patient and SO personally.
- Rationale: Assists patient and SO to accept body changes and feel all right about self. Anger is most often directed at the situation and lack of control individual has over what has happened (powerlessness), not with the individual caregiver.
- Ascertain patient’s desire to visit with a person with an ostomy. Make arrangements for visit, if desired.
- Rationale: A person who is living with an ostomy can be a good support system/role model. Helps reinforce teaching (shared experiences) and facilitates acceptance of change as patient realizes “life does go on” and can be relatively normal.
Nursing Diagnosis
- Skin Integrity, risk for impaired
Risk factors may include
- Absence of sphincter at stoma
- Character/flow of effluent and flatus from stoma
- Reaction to product/chemicals; improper fitting/care of appliance/skin
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired Outcomes
- Maintain skin integrity around stoma.
- Identify individual risk factors.
- Demonstrate behaviors/techniques to promote healing/prevent skin breakdown.
Nursing Interventions
- Inspect stoma and peristomal skin area with each pouch change. Note irritation, bruises (dark, bluish color), rashes
- Rationale: Monitors healing process and effectiveness of appliances and identifies areas of concern, need for further evaluation and intervention. Early identification of stomal necrosis or ischemia or fungal infection (from changes in normal bowel flora) provides for timely interventions to prevent serious complications. Stoma should be red and moist. Ulcerated areas on stoma may be from a pouch opening that is too small or a faceplate that cuts into stoma. In patients with an ileostomy, the effluent is rich in enzymes, increasing the likelihood of skin irritation. In patient with a colostomy, skin care is not as great a concern because the enzymes are no longer present in the effluent.
- Clean with warm water and pat dry. Use soap only if area is covered with sticky stool. If paste has collected on the skin, let it dry, then peel it off.
- Rationale: Maintaining a clean and dry area helps prevent skin breakdown.
- Measure stoma periodically: at least weekly for first 6 wk, then once a month for 6 mo. Measure both width and length of stoma.
- Rationale: As postoperative edema resolves (during first 6 wk), the stoma shrinks and size of appliance must be altered to ensure proper fit so that effluent is collected as it flows from the ostomy and contact with the skin is prevented.
- Verify that opening on adhesive backing of pouch is at least 1⁄16 to 1⁄8 in (2–3 mm) larger than the base of the stoma, with adequate adhesiveness left to apply pouch.
- Rationale: Prevents trauma to the stoma tissue and protects the peristomal skin. Adequate adhesive area prevents the skin barrier wafer from being too tight. Note: Too tight a fit may cause stomal edema or stenosis.
- Use a transparent, odor-proof drainable pouch.
- Rationale: A transparent appliance during first 4–6 wk allows easy observation of stoma without necessity of removing pouch/irritating skin.
- Apply appropriate skin barrier: hydrocolloid wafer, karaya gun, extended-wear skin barrier, or similar products.
- Rationale: Protects skin from pouch adhesive, enhances adhesiveness of pouch, and facilitates removal of pouch when necessary. Note: Sigmoid colostomy may not require use of a skin barrier once stool becomes formed and elimination is regulated through irrigation.
- Empty, irrigate, and cleanse ostomy pouch on a routine basis, using appropriate equipment.
- Rationale: Frequent pouch changes are irritating to the skin and should be avoided. Emptying and rinsing the pouch with the proper solution not only removes bacteria and odor-causing stool and flatus but also deodorizes the pouch.
- Support surrounding skin when gently removing appliance. Apply adhesive removers as indicated, then wash thoroughly.
- Rationale: Prevents tissue irritation or destruction associated with “pulling” pouch off.
- Investigate reports of burning, itching, or blistering around stoma.
- Rationale: Indicative of effluent leakage with peristomal irritation, or possibly Candida infection, requiring intervention.
- Evaluate adhesive product and appliance fit on ongoing basis.
- Rationale: Provides opportunity for problem solving. Determines need for further intervention.
- Consult with certified wound, ostomy, continence nurse.
- Rationale: Helpful in choosing products appropriate for patient’s particular rehabilitation needs, including type of ostomy, physical/mental status, abilities to handle self-care, and financial resources.
- Apply corticosteroid aerosol spray and prescribed antifungal powder as indicated.
- Rationale: Assists in healing if peristomal irritation persists and/or fungal infection develops. Note: These products can have potent side effects and should be used sparingly.
Other Reference:

