Notes

Description
- Preterm labor is labor that begins after 20 weeks’ gestation and before 37 weeks’ gestation.
Etiology
- Among the many causes of preterm labor are:
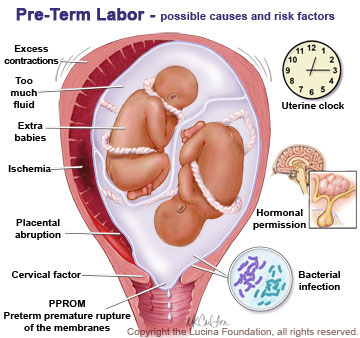
- PROM
- Preeclampsia
- Hydramnios
- Placenta previa
- Abruptio placentae
- Incompetent cervix
- Trauma
- Uterine structural anomalies
- Multiple gestation
- Intrauterine infection (chorioamnionitis)
- Congenital adrenal hyperplasia
- Fetal death
- Maternal factors, such as stress (physical and emotional), urinary tract infections, and dehydration.
Pathophysiology
- The uterus begins the process of contraction prior to term gestational age.
Assessment Findings
- Clinical manifestations of preterm labor are basically the signs of true labor that occur when the gestational age of the fetus is greater than 20 and less than 37 weeks.
- Low back pain
- Suprapubic pressure
- Vaginal pressure
- Rhythmic uterine contractions
- Cervical dilation and effacement
- Possible rupture of membranes
- Expulsion of the cervical mucus plug
- Bloody show
Nursing Management
1. Assess the mother’s condition and evaluate signs of labor.
- Obtain a thorough obstetric history.
- Obtain specimens for complete blood count and urinalysis.
- Determine frequency, duration, and intensity uterine contractions.
- Determine cervical dilation and effacement.
- Assess status of membranes and bloody show.
2. Evaluate the fetus for distress, size, and maturity (sonography and lecithin-sphingomyelin ratio)
3. Perform measures to manage or stop preterm labor.
- Place the client on bed rest in the side-lying position.
- Prepare for possible ultrasonography, amniocentesis, tocolytic drug therapy, and steroid therapy.
- Administer tocolytic (contraction-inhibiting) medications as prescribed.
- Assess for side effects of tocolytic therapy (e.g., decreased maternal blood pressure, dyspnea, chest pain, and FHR exceeding 180 beats/min).
4. Provide physical and emotional support. Provide adequate hydration.
5. Provide client and family education.
Exam
Nursing Care Plan
Risk for [Fetal] Injury
Risk for Injury: Vulnerable for injury as a result of environmental conditions interacting with the individual’s adaptive and defensive resources, which may compromise health.
Risk factors
- Delivery of preterm infant
Possibly evidenced by
- [Not applicable]
Desired Outcomes
- Patient will maintain pregnancy at least to the point of fetal maturity.
| Nursing Interventions | Rationale |
|---|---|
| Assess for maternal conditions that would contraindicate steroid therapy to facilitate fetal lung maturity. | In PIH and chorioamnionitis, steroid therapy may aggravate hypertension and mask signs of infection. Steroids may increase serum glucose levels in the patient with diabetes. Drug will not be effective if unable to delay birth for at least 48 hours. |
| Assess FHR; note presence of uterine activity or cervical changes. Prepare to possible preterm delivery. | Tocolytics can increase FHR. Delivery may be extremely rapid with small infant if persistent uterine contractions are unresponsive to tocolytics, or if cervical changes continue. |
| Provide information about the actions and side effects of the drug therapy. | Important for the client or couple to know the purpose of the drugs being administered:
|
| Review potential side effects of steroid therapy with client or couple. | Short-term effects may include hypoglycemia, increased risk of sepsis, and possible suppression of aldosterone for 2 weeks following delivery. |
| Stress necessity of follow-up care. | If fetus is not delivered within 7 days of administration of steroids, dose should be repeated weekly. |
| Assist as needed with analysis of amniotic fluid from amniocentesis or vaginal pool specimen; test for ferning. | L/S ratio, presence of PG, and shake test results indicate fetal lung status. Ferning indicates rupture of membranes with increased risk of infection. |
| Administer betamethasone (Celestone) deep IM. | Betamethasone is a synthetic cortisol that can accelerate fetal lung maturity by stimulating surfactant production and thereby preventing or decreasing the severity of respiratory distress syndrome. Administration into the deltoid muscle may result in local atrophy. |
| Administer antibiotics, as indicated. | In the event of PROM and fetal lung immaturity, antibiotics may be used to prevent or reduce risk of infection, while allowing an additional 24 hours to elapse after administration of Celestone. |
| Initiate tocolytic therapy, as ordered. | Helps reduce myometrial activity to prevent or delay early delivery. |
Acute Pain
Acute Pain: Unpleasant sensory and emotional experience arising from actual or potential tissue damage or described in terms of such damage; sudden or slow onset of any intensity from mild to severe with anticipated or predictable end and a duration of <6 months.
May be related to
- Muscle contraction (uterine contractions)
- Effect of medications
Possibly evidenced by
- Reports of pain or discomfort
- Muscle tension
- Narrowed focus
Desired Outcomes
- Patient will report discomfort is minimized or controlled.
- Patient will use relaxation techniques, effectively.
- Patient will appear relaxed and will rest appropriately.
| Nursing Interventions | Rationale |
|---|---|
| Expedite the admission process and initiate bedrest for client, using lateral recumbent position. | Side-lying position improves uterine blood flow and may decrease uterine irritability. |
| Teach relaxation techniques (e.g., deep breathing exercises, visualization, guided imagery, soft music). | Help client refocus, attention decreases muscle tension, reduces perception of discomfort and promotes sense of control. |
| Using nursing comfort measures such as changes of linen and position, back rubs, and therapeutic touch. | Relieves muscle tension and fatigue. |
| Encourage routine inspection of mucous membranes for ulceration or reaction to chewing of nifedipine, if used. | Nifedipine may be irritating to the oral cavity in which case it should be swallowed whole. |
| Monitor maternal and fetal vital signs. | Reflects effectiveness of interventions. |
| Administer analgesics, as indicated. | Mild analgesics decreases muscle tension and discomfort. |
Deficient Knowledge
Deficient Knowledge: Absence or deficiency of cognitive information related to specific topic.
May be related to
- Misinterpretation or lack of information
Possibly evidenced by
- Request for information
- Verbalization of misconceptions
Desired Outcomes
- Patient will verbalize awareness of implications and possible outcomes of preterm labor.
- Patient will identify signs and symptoms requiring evaluation and intervention.
- Patient will demonstrate understanding of home therapy and/or self-care needs.
| Nursing Interventions | Rationale |
|---|---|
| Ascertain client’s knowledge about preterm labor and possible outcomes. | Establishes baseline assessment and identifies needs. |
| Assess client readiness to learn. | Factors such as anxiety or lack of awareness of need for information can interfere with readiness to learn. Retention of information is enhanced when client is motivated and ready to learn. |
| Include significant others in teaching learning process. | Support from significant others can help allay anxiety as well as reinforce principles of teaching and learning. |
| Provide information about follow-up care when client is discharged. | Client may need to return on a regular basis for monitoring and/or treatments. |
| Identify signs and/or symptoms that should be reported immediately to the healthcare provider (e.g, sustained uterine contractions, clear drainage from vagina, bleeding). | Prompt evaluation and interventions may improve the outcome of the pregnancy and avert complications. |
| With the client, review the signs and symptoms of early labor. | Helps the client to recognize preterm labor so therapy can be instituted or reinstituted promptly. |
| Demonstrate how client is to evaluate contraction activity after discharge (e.g., lying down, tilted to the side with a pillow to the back, placing fingertips on the fundus for approximately 1 hour to note hardening or tightening of the uterus). | Although uterine contractions commonly occur periodically, contractions occurring 10 mins or less apart for an hour can result in cervical dilation and labor without prompt intervention. Self-monitoring is usually adequate and has no cost; however, some healthcare providers may require electronic monitoring, which necessitates data be transmitted via telephone lines and interpreted by a nurse upon receipt. |
| Stress importance of maintaining daily record of uterine activity and other pertinent information as individually appropriate. | Periodic review of data will be used to adjust therapy. |
| Arrange for client to visit neonatal intensive care unit. | Helps alleviate fears and facilitates adjustments to situation. |
| Discuss need to restrict lifestyle by stopping smoking and probably by restricting sexual activity and nipple stimulation. | Nicotine has adverse effect on fetoplacental growth and on uterine circulation. Organism or release of oxytocin(from nipple stimulation) may stimulate uterine activity. |
| Encourage regular rest periods 2-3 times a day in side-lying position. If bedrest is to be continued after discharge, suggest client spend part of day on couch or recliner. | Enhances relaxation and reduces fatigue. If client is up and about, resting in the bedroom may maximize rest. |
| Review daily routine, employment, and activity schedule to identify alternatives and ways to compensate for limitations. | Pacing activities, avoidance of heavy chores, lifting, and modification in work duties or cessation of employment may help prevent recurrence of preterm labor. |
| Determine availability and level of commitment of supportive resources. | Division of home care responsibilities helps reduce risk of caregiver burnout when one individual attempts to take on responsibilities of the client in addition to own role. |
| Advise client to empty bladder every two (2) hours while awake. | Prevents pressure of a full bladder on the irritable uterus. |
| Review daily fluid need; avoid coffee. | Dehydration and caffeine both lead to increased uterine muscle irritability. |
| Stress avoidance of OTC drugs while tocolytic agents are being administered unless approved by physician. | Concurrent use of OTC drugs may cause deleterious effects, especially if OTC drug has similar side effects to tocolytic agents. |
| Recommend adhering to predetermined schedule for oral drug therapy. | Maintains blood level of drug for optimum effect. |
| Provide information about taking oral tocolytics with food. | Food improves tolerance to drug and reduces side effects. |
| Instruct in proper use of infusion pump when use and need to count and/or record pulse before bolus doses are administered. | Promotes safe use of drug, enhances participation in therapeutic regimen and supports self-care and independence. |
| Identify drug side effects requiring medical evaluation. | Pulse rate greater than 120 bpm; presence of tremors, palpitations, chest pain, or dyspnea, or feeligns of nervouseness, and agitation may require alterations or discontinuiation of drug. |
| Establish routine schedule for homecare nurse visitation. Provide regular telephone contact. | Weekly or biweekly visits provide opportunity for regular physical assessment, review of uterine activity record, and additional information for education. |
Anxiety
Anxiety: Vague uneasy feeling of discomfort or dread accompanied by an autonomic response.
May be related to
- Situational crisis
- Perceived or actual threats to self and fetus
Possibly evidenced by
- Increasing tension
- Apprehension
- Sympathetic stimulation
Desired Outcomes
- Patient will verbalize understanding of individual situation and possible outcomes
- Patient will report anxiety is reduced and/or manageable
- Patient will appear relaxed; with maternal vital signs within normal limits.
| Nursing Interventions | Rationale |
|---|---|
| Explain the procedures, nursing interventions, and treatment regimen. Keep communication open; discuss with the client the possible side effects and outcomes while maintaining an optimistic attitude. | Information and knowledge of the reasons of these activities can decrease fear of the unknown. |
| Orient client and partner to labor suite environment | Helps client and/or significant others feel at ease and more comfortable in their surroundings. |
| Answer questions honestly, especially information regarding contraction pattern and fetal status. | Provision of clear information can help the client or couple understand what is happening and may reduce anxiety. |
| Encourage use of relaxation techniques. | Enables the client to obtain maximum benefit from rest periods; prevents muscle fatigue and improves uterine blood flow. |
| Encourage verbalization of fears or concerns. | Can help reduce anxiety and stimulate identification of coping behaviors. |
| Monitor maternal and fetal vital signs. | Vital signs of client and fetus may be altered by anxiety. Stabilization may reflect reduction anxiety level. |
| Assess support systems available to the client or couple, whether the client remains hospitalized or is to return home to await delivery. | The assistance and caring of significant others, including caregivers, are extremely important during this time of uncertainty and stress. If the client is to return home, additional support will be required to meet self-care needs and homemaker activities as well as child care, as appropriate. |
| Administer sedative if other measures are not successful. | Provides soothing and tranquilizing effect. |
Activity Intolerance
Activity Intolerance: Insufficient physiologic or physiological energy to endure or complete required or desired activity.
May be related to
- Prolonged physical activity and stress
- Muscle hypersensitivity
Possibly evidenced by
- Continued uterine contractions and/or irritability
- Reduced activity level
Desired Outcomes
- Identify and/or engage in activities appropriate to situation.
- Demonstrate reduction and/or cessation of uterine contractions.
| Nursing Interventions | Rationale |
|---|---|
| Provide comforts measures (e.g., back rubs, changes of position, decreased stimuli in room) | Decreases muscle tension and fatigue and helps promote sense of well-being. |
| Explain the reasons of requiring bedrest. Use lateral recumbent (i.e., side-lying position) and decrease activity. | These measures are intended to keep the fetus off the cervix and may enhance uterine perfusion, bedrest may decrease uterine irritability. |
| Cluster nursing care: group activities together as much as possible, such as medication administration, vital signs, and assessment. | Promotes longer opportunities for client to rest between interruptions. |
| Provide uninterrupted periods for rest and/or sleep. | Helps promote rest, prevent fatigue, and may enhance relaxation. |
| Offer diversional activities (e.g., reading, watching TV) | Assist client in coping with decreased activity. |
| Assess uterine contractions per protocol. | Reflects effectiveness of and determines need for further interventions. |
Risk for Poisoning
Risk for Poisoning: Vulnerable for accidental exposure to or ingestion of drugs or dangerous products in sufficient doses that may compromise health.
Risk factors
- Dose-related and toxic or side effects of tocolytics
Possibly evidenced by
- Not applicable.
Desired Outcomes
- Patient will display no evidence of untoward effects of tocolytic therapy.
- Patient will prevent or minimize maternal injury.
- Patient will demonstrate cessation of uterine contractions, dependent of fetal well-being.
| Nursing Interventions | Rationale |
|---|---|
| Place client in lateral recumbent position. Elevate head during infusion of IV drug. | Decreases uterine irritability, increases placental perfusion and reduces supine hypotension. |
| Monitor vital signs. Auscultate lung sounds, investigate cardiac irregularities, and investigate reports of dyspnea and/or chest tightness. | Complications, such as pulmonary edema, cardiac arrhythmia, agitation, dyspnea, and chest pain may occur with administration of beta-receptor agonist such as terbutaline sulfate (Brethine) or ritodrine (Yutopar). |
| Measure intake and output. Encourage fluid intake between 2,000 and 3,000 ml/day, unless contraindicated (e.g., during administration of magnesium sulfate). | Promotes adequate hydration and prevents fluid excess, especially when magnesium sulfate is administered which is excreted through the kidneys, therefore urine output must be maintained. |
| Weight client daily. | Detects potential alteration in urinary functioning and/or retention of fluid. |
| Monitor for drowsiness, hot flashes, visual disturbances, respiratory depression, and depressed tendon reflexes. | Indicates neuromuscular depression, indicating increasing serum levels of magnesium sulfate. |
Have antidotes readily available:
|
Administration of antidote may be necessary to reverse or counteract effects of tocolytic agents. |
| Assist as needed with sterile vaginal examination. Vaginal examinations should be kept to a minimum. | To assess cervical status. Vaginal examinations are kept to a minimum because they may contribute to uterine irritability and infection. |
| Administer IV solution or fluid bolus as indicated. | Hydration may decrease uterine activity. Before beginning drug therapy, hydration promotes renal clearance and minimizes hypotension. |
| Administer IV solutions containing tocolytic agents (e.g., magnesium sulfate, terbutaline sulfate) by infusion pumps or microdrip equipment, or by subcutaneous route. | Magnesium sulfate acts directly on myometrial tissue to promote relaxation; therefore, there are fewer side effects than other drug choices.Terbutaline sulfate relaxes uterine muscle as well as bronchioles and blood vessel walls. |
| Obtain serum potassium level prior to initiation of IV terbutaline and periodically per protocol. Monitor serum glucose and potassium levels. | Terbutaline sulfate cause movement of potassium ions into cells, decreasing plasma levels; elevated blood glucose and plasma insulin levels, and release of glycogen from muscle and liver may result in hyperglycemia. |
| Administer nifedipine (Procardia) to be chewed and swallowed with food or drink. Nifedipine may occasionally be alternated with terbutaline sulfate. | Nifedipine, a calcium channel blocker, has been used experimentally when other drugs fail to suppress uterine activity. |
| Monitor nifedipine levels. Note development of tachycardia, hypotension, peripheral edema, or proteinuria. | The therapeutic dosage of nifedipine for preterm labor has not been established. Periodic monitoring may avert or prevent development of adverse effects (e.g., heart failure). |
| Apply antiembolic hose as indicated, and provide passive range of motion exercises to legs every 1-2 hours. | Prevents pooling of blood in lower extremities, which can occur because of smooth muscle relaxation. |
| Monitor serum magnesium levels per protocol during administration of magnesium sulfate. | Therapeutic level is 4-7 mEq/L, or 6-8 mg/dL. Toxic signs and symptoms develop above 10 mg/dL. |
| Insert indwelling catheter, as indicated. | Urine output must be monitored and maintained when administering magnesium sulfate. Output should be at least 30 ml/hr, or 100 ml in a 4-hour period. |
| Assess uterine contractions and FHR electronically while IV tocolytics are administered, or at least twice a day when oral route is used. | Tactile electronic monitoring of uterine contractions and FHS provides a continuous fetal/uterine assessment and basis for altering or maintaining rate of drug administration. |
| Decrease IV dose of tocolytics and gradually wean client to subcutaneous or oral dose, as indicated. | IV therapy should continue at least 12 hour after contraction cease. Oral or subcutaneous therapy should begin 30 mins before stopping IV infusion. |