Notes

Description
- In this surgical procedure, the newborn is delivered through the abdomen from an incision made through the maternal abdomen and the uterine myometrium.
- The surgery may be preplanned (elective) or arise from an unanticipated problem.
- Two incisions are made: one in the abdominal wall (skin incision) and the other in the uterine wall. Either of two skin incisions is used: a midline vertical incision between the umbilicus and the symphysis or a Pfannenstiel incision just above the symphysis (Fig. 1). Three types of uterine incisions are possible (Fig. 2): (1) low transverse; (2) low vertical; and (3) classic, a vertical incision into the upper uterus. The low transverse uterine incision is preferred unless a very large fetus or placenta previa in the lower uterus prevents its use. The uterine incision does not always match the skin incision. For example, a woman may have a vertical skin incision and a low transverse uterine incision, particularly if she is very obese.
- In subsequent pregnancies and delivery, a trial of labor and vaginal birth is increasingly regarded as safe and appropriate as long as cephalopelvic disproportion does not exist and the previous incision was low transverse.
- Elective, repeat cesarean may be performed in the absence of a specific indication for operative delivery when either the physician or the client is unwilling to attempt vaginal delivery.
- Anesthesia may be general, spinal, or epidural; preoperative and postoperative care will vary accordingly.
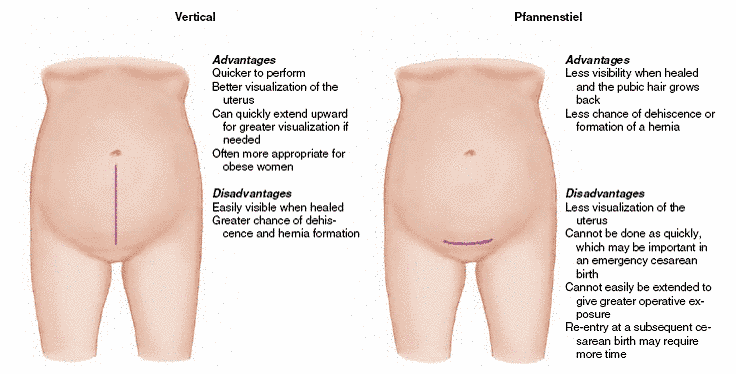
Skin (abdominal wall) incisions for cesarean birth.
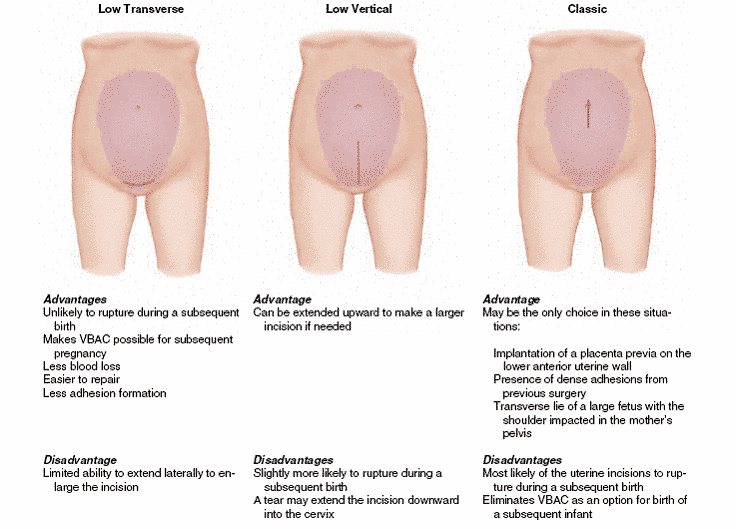
Uterine incisions for cesarean birth. The abdominal and uterine incisions do not always match. VBAC, Vaginal birth after cesarean
Positioning
- Supine, with a small roll under the right hip (to reduce vena cava compression); arms extended on armboards.
Incision sites
- Classic approach, vertical (low midline).
Packs/drapes
- Extra drape sheet
- Towels
- Receiving pack for baby
Instrumentation
- C-section tray
- Delivery forceps
- Cord clamp
Supplies/ Equipment
- Basin set
- Blades
- Suction
- Neonatal receiving unit
- Self-contained oxygen
- I.D bands
- Bulb syringe
- Solutions
- Sutures
Procedure
- Using the appropriate incisions, consistent with the estimated size of the fetus, the abdomen is opened, the rectus muscle are separated, and the peritoneum incised (similar to an abdominal hysterectomy), exposing the distended uterus.
- Large vessels are clamped or cauterized, but usually no attempt to control hemostasis is made since it may delay delivery time ( 3-5 minutes after initial incision is ideal).
- The scrub person must be ready with suction, dry laps, and a bulb syringe.
- The bladder is retracted downward with the bladder blade of the balfour retractor and a small incision is made with the second knife and extended with a bandage scissors (blunt tip prevents injury to the baby’s head).
- The amniotic sac is entered and immediately aspirated the fluid.
- The bladder blade is removed, and the assistant will push on the patient’s upper abdomen while the surgeon simultaneously delivers the infant’s head in an upward position.
- The baby’s airways are suctioned with the bulb syringe, and the baby is completely delivered and placed upon the mother’s abdomen.
- The umbilical cord is double clamped and cut.
- The baby is wrapped in a sterile receiving blanket and transferred to the warming unit for immediate assessment and care.
- Once the bay has been safely delivered, the emergent phase of the procedure has been ended.
- Using a nonecrushing clamp, the uterine wall is grasped for traction during closure.
- The closure is performed in two layers with a heavy absorbable suture, using a continuous stitch, the second overlapping the first.
- Following closure of the uterus, the bladder flap is reperitonealized with a running suture, and the uterus is pushed back inside the pelvic cavity.
- The cavity is irrigated with warm saline, and closed in layers.
- Skin is closed with the surgeon’s preference. If a tubal ligation is to be performed, it is done prior to the abdominal closure sequence.
Perioperative Nursing Considerations
- A C-section requires an additional uterine count of sponges, sharps, and instruments prior to its closure.
- Oxytocin should be available for the anesthesiologist to administer I.V.
- Once the uterus is opened, immediate suctioning is necessary.
- A warm, portable isolette should be available to transport the infant to the newborn nursery.
Reasons For Performing A Cesarean Delivery
1. Maternal factors
- Cephalopelvic disproportion (CPD)
- Active genital herpes or papilloma
- Previous cesarean birth by classic incision
- Presence of severe disabling hypertension or heart disease
2. Placental factors
- Placenta previa
- Abruptio placental
3. Fetal factors
- Transverse fetal lie
- Extreme low birth weight
- Fetal distress
- Compound conditions, such as macrosomia and transverse lie.
Nursing Management
1. Perform a complete maternal and fetal assessment.
- Obtain a complete obstetric history.
- If he client presents with labor determine frequency, duration, and intensity of contractions.
- Determine the condition of the fetus through fetal heart tones, fetal monitoring strips, fetal scalp blood sample, fetal activity changes, and presence of meconium in amniotic fluid.
2. Prepare the client for cesarean delivery in the same way whether the surgery is elective or emergency. Depending on hospital policy:
- Shave or clip pubic hair.
- Insert a retention catheter to empty the bladder continuously.
- As prescribed, insert intravenous lines, collect specimens for laboratory analysis, and administer preoperative medications.
- Also as prescribed, provide an antacid (to prevent vomiting and possible aspiration of gastric secretions) and prophylactic antibiotics (to prevent endometritis).
- Assist the client to remove jewelry, dentures, and nail polish, as appropriate.
- As needed, reinforce the obstetrician’s explanation of the surgery, the expected outcome, and the anesthesiologist’s explanation of the kind of anesthetics to be used (depending on the client’s cardiopulmonary status).
- Make sure the client’s signed informed consent is on file.
- Continue assessing maternal and fetal vital signs in accordance with hospital policy until the client is transported to the operating room.
- Notify other health care team members of the pending delivery.
- Modify preoperative teaching to meet the needs of planned versus emergency cesarean birth; depth and breadth of instruction will depend on the circumstances and time available.
- If there is time, begin explaining what the client can expect postoperatively. Discuss pain relief, turning, coughing, deep breathing, and ambulation.
- Inform the client that intraoperative and postpartum care will be performed by the surgical and obstetric team, and that the newborn will receive care by the pediatrician and a nurse skilled in neonatal care procedures (ie, resuscitation).
3. Facilitate a family- centered cesarean birth by including , when possible, such activities as:
- Preparing the partner for participation in the delivery.
- Reuniting the family as soon as possible following delivery.
- Providing for family time alone in the critical first hours after the mother and newborn are stabilized.
- Including the father and siblings (as possible) when demonstrating care of the newborn.
- Encouraging the mother’s support person to remain with her as much as possible. In some cases, this person may accompany the client to the surgical suite and stay with her throughout the birth.
4. Provide physical and emotional support.
- Anticipate parental feelings of “failure” related to cesarean rather than “normal” birth. In such a situation, provide time for them to relive and talk through the experience. Offer reassurance and support.
- Assist the family in planning for care of mother and newborn at home (Client and Family Teaching- Table 1)
Table 1
Client and Family Teaching
Explain to the mother, her partner, and other family members that recovery from a surgical cesarean delivery is slower, and often more painful, when compared with recovery from a normal vaginal delivery. The following considerations must be taken into account:
|
Exam
Nursing Care Plan
Risk for Acute Pain
Risk for Acute Pain: Defined as an increased risk of having an unpleasant sensory and emotional experience arising from potential tissue damage.
Risk factors may include
- Increased muscle contractions
- Psychological reactions
Possibly evidenced by
- [Not applicable; presence of signs/symptoms establishes an actual diagnosis]
Desired Outcomes
- Patient verbalizes reduced discomfort or pain.
| Nursing Interventions | Rationale |
|---|---|
| Assess location, nature, and duration of pain, especially as it relates to the indication for cesarean birth. | Indicates the suitable choice of treatment. The patient awaiting imminent cesarean birth may encounter varying degrees of discomfort, depending on the indication for the procedure, e.g., failed induction, dystocia. |
| Drop anxiety-producing circumstance (e.g., loss of control), give accurate information, and encourage presence of partner. | Levels of pain tolerance are individual and are affected by various factors. Extreme anxiety following an emergency situation may develop discomfort due to fear, tension, and pain affecting the patient’s ability to cope. |
| Educate proper relaxation techniques; position for comfort as possible. Use Therapeutic Touch, as appropriate. | May help in decreasing anxiety and tension, promote comfort and enhance sense of well-being. |
| If indicated, administer medications such as sedative, narcotics, or preoperative drugs. | Promotes comfort by blocking pain impulses. Potentiates the action of anesthetic agents. |
Risk for Infection
Risk for Infection: At increased risk for being invaded by pathogenic organisms.
Risk factors may include
- Invasive procedures
- Rupture of amniotic membranes
- Break in the skin
- Decreased Hb
- Exposure to pathogens
Possibly evidenced by
- [Not applicable; presence of signs/symptoms establishes an
actual diagnosis]
Desired Outcomes
- Patient is free from infection
- Patient achieves timely wound healing without complications.
| Nursing Interventions | Rationale |
|---|---|
| Know history for preexisting conditions or risk factors. Note time of rupture of membranes. | History of diabetes or hemorrhage increase chances of infection and poor wound healing. Risk of chorioamnionitis increases with the passage of time, placing mother and fetus at risk. Presence of infectious process may increase fetal risk of contamination |
| Assess signs and symptoms of infection (e.g., elevated temperature, pulse, WBC; abnormal odor or color of vaginal discharge, or fetal tachycardia). | Rupture of membranes occurring 24 hr before the surgery may result in chorioamnionitis prior to surgical intervention and may impair wound healing. |
| Provide perineal care per protocol, particularly once membranes have ruptured. | Decreases risk of ascending infection. |
| Carry out preoperative skin preparation; scrub according to protocol. | Decreases risk of skin contaminants entering the operative site, reducing risk of preoperative infection. |
| Take blood, vaginal, and placental cultures, as indicated. | Determines infecting organism and degree of involvement. |
| Record Hb and Hct, and estimated blood loss during surgical procedure. | Risk of postdelivery infection and poor healing is increased if Hb levels are low and blood loss is excessive. Note: Greater blood loss is associated with classic incision than with lower uterine segment incision. |
| Give parenteral broad-spectrum antibiotic preoperatively. | Prophylactic antibiotic may be requested to prevent development of an infectious process, or as treatment for an identified infection, especially if the patient has had prolonged rupture of membranes. Note: Research suggests administration of antibiotic up to 2 hr before start of procedure provides the most protection from infection |
Risk for Impaired Fetal Gas Exchange
Risk for Impaired Fetal Gas Exchange: At risk for excess or deficit in oxygenation and/or carbon dioxide elimination at the alveolar-capillary membrane.
Risk factors may include
- Altered blood flow to placenta and/or through umbilical cord
Possibly evidenced by
- [Not applicable; presence of signs/symptoms establishes an
actual diagnosis]
Desired Outcomes
- Patient displays optimal FHR.
- Patient manifests normal variability on monitor strip.
- Patient reduces frequency of late or prolonged variable decelerations.
| Nursing Interventions | Rationale |
|---|---|
| Note presence of maternal factors that negatively affect placental circulation and fetal oxygenation. | Decreased circulating volume or vasospasms within the placenta decrease oxygen available for fetal uptake. |
| Record FHR, note any changes or decelerations during and following contractions. | Owing to hypoxia, fetal distress may transpire; may be displayed by reduced variability, late decelerations, and tachycardia followed by bradycardia. Note: Infection from prolonged rupture of membranes also increases FHR. |
| Record presence of variable decelerations; change patient’s position from side to side. | Compression of cord between birth canal and presenting part may be relieved by position changes. |
| Examine color and amount of amniotic fluid when membranes rupture. | Fetal distress in vertex presentation is manifested by meconium staining, which is the result of a vagal response to hypoxia. |
| Auscultate FHR when membranes rupture. | In the absence of full cervical dilation, occult or visible prolapse of the umbilical cord may necessitate cesarean birth. |
| Monitor fetal heart response to preoperative medications or regional anesthesia. | Narcotics normally reduce FHR variability and may necessitate administration of naloxone (Narcan) following delivery to reverse narcotic-induced respiratory depression. Maternal hypotension in response to anesthesia usually causes transient fetal bradycardia, reduced variability, and sleep. |
| Apply internal lead, and monitor fetus electronically as indicated. | Give more precise measurement of fetal response and condition. |
| Give supplemental oxygen to mother via mask. | Maximizes oxygen available for placental uptake. |
| Give IV fluid bolus prior to initiation of epidural or spinal anesthesia. | Optimizes uteroplacental perfusion, helps prevent hypotensive response. |
| Help physician with elevation of vertex, if required. | Position changes may reduce pressure on cord. |
| Plan the presence of pediatrician and neonatal intensive care nurse in delivery room for both scheduled and emergency cesarean births. | Owing to underlying maternal condition(s) and alternative birth process, infant may be preterm or may experience altered responses, necessitating immediate care or resuscitation. |
Risk for Maternal Injury
Risk for Maternal Injury: Vulnerable for injury as a result of environmental conditions interacting with the individual’s adaptive and defensive resources, which may compromise health.
Risk factors may include
- Altered mobility
- Decreased sensation
- Delayed gastric motility
- Effects of medication
- Traumatized tissue
Possibly evidenced by
- [Not applicable; presence of signs/symptoms establishes an
actual diagnosis]
Desired Outcomes
- Patient is free of injury.
| Nursing Interventions | Rationale |
|---|---|
| Remove prosthetic devices (e.g., contact lenses, dentures or bridges) and jewelry. | Lessens risk of accidental injury. |
| Determine time and content of last meal. Report information to anesthesiologist. Ensure availability and functioning of resuscitation equipment. | If patient has eaten just before surgical procedure, risks of vomiting and aspiration increase, and general anesthesia may be contraindicated. |
| Restrict oral intake once decision for cesarean birth is made. | Reduces pssibility of aspiration from vomiting. |
| Review labor record, noting voiding frequency, output, appearance, and time of last voiding. | May signify urine retention or reflect fluid imbalance or dehydration in patient who has been in prolonged labor. |
| Monitor urine output and color following insertion of indwelling catheter. Note any blood-tinged urine. | Reveals hydration level, circulatory status, and possible bladder trauma associated with surgical procedure. |
| Assist with positioning for anesthesia; support legs in postoperative transfer to stretcher. Note patient’s response during and after anesthesia. | Necessary for placement of anesthesia. Patient with epidural or spinal anesthesia may acquire weakness or decreased sensation of lower extremities. Idiosyncratic responses to anesthesia can transpire, such as anaphylaxis or respiratory paralysis if anesthetic block rises too high. |
| Maintain specific instrument and sponge counts at critical times during closure, according to hospital protocol. | Guarantees that all equipment and sponges are accounted for and not accidentally left in patient’s body. |
| Get urine specimen for routine analysis, protein, and specific gravity. Ensure that laboratory results are available before surgery is started. | Patient is at increased risk if infectious process or hypertensive state is present. |
| Insert indwelling catheter to continuous gravity drainage system either just before surgical procedure or in the operating room, as indicated | Reduces risk of bladder injury during surgical procedure. |
| Give preprocedural medication (e.g, atropine). | Reduces oral secretions, limiting risk of aspiration. |
Risk for Decreased Cardiac Output
Risk for Decreased Cardiac Output: At risk for inadequate blood pumped by the heart to meet metabolic demands of the body.
Risk factors may include
- Alteration in systemic vascular resistance
- Decreased venous return
Possibly evidenced by
- [Not applicable; presence of signs/symptoms establishes an
actual diagnosis]
Desired Outcomes
- Patient remains normotensive, with blood loss less than 800 ml.
| Nursing Interventions | Rationale |
|---|---|
| Record length of labor, if applicable. Assess for dehydration or excess intrapartal fluid losses. | Decreased intake and/or increased fluid losses lead to reduced circulating volume and cardiac output. |
| Remove nail polish on fingernails/toes. | Essential for clear visualization of nailbeds for assessing circulatory status. |
| Check respirations, BP, and pulse before, during, and after administration of anesthesia. | Hypotension is an expected side effect of regional anesthesia (e.g., epidural or spinal anesthesia) because such anesthesia relaxes smooth muscles within vascular walls, affecting circulating volume and reducing placental perfusion. |
| Place towel or wedge under patient’s hip. | Shifts uterus off inferior vena cava and increases venous return. Compression caused by obstruction of the inferior vena cava and aorta by the gravid uterus in a supine position may cause as much as a 50%decrease in cardiac output. |
| Note shift in behavior or mental status, cyanosis of mucous membranes. | Oxygen deficits are manifested first by changes in mental status, later by cyanosis. |
| Give supplemental oxygen via mask, as indicated. | Increases oxygen available for maternal and fetal uptake. Note: Nasal cannula is not recommended because of excessive oxygen loss to environment. |
| Initiate IV infusion of electrolyte solution. Administer bolus, as indicated. | Expands circulatory volume, especially prior to administration of epidural or spinal anesthesia; provides route for emergency medication in the event of a complication. |
| Note alteration in vital signs; assist anesthetist as needed. Estimate and record blood losses. | Excess fluid losses and hemorrhage during labor and the intraoperative period may reduce cardiac output and promote vasoconstriction with shunting of blood to major organs. Diminished cardiac output and shock are manifested by decreased BP, increased or thready pulse, and cool or clammy skin. |
| Administer whole blood, plasma expanders, cryoprecipitate, platelets, or packed cells as indicated. | Replaces fluid losses, increases circulating blood volume, and increases oxygen-carrying capacity. |
| Prepare and administer oxytocin (Pitocin) infusion. | Once delivery of infant and placenta is completed, Pitocin aids myometrium contraction and reduces blood loss from exposed endometrial blood vessels. |
Sensory/Perceptual Alterations
Sensory/Perceptual Alterations: Change in the amount or patterning of incoming stimuli accompanied by a diminished, exaggerated, distorted, or impaired response to stimuli.
May be related to
- Multiple environmental stimuli
- Increased number of personnel
- Excessive noise level
- Psychological stress
Possibly evidenced by
- Exaggerated emotional response
- Irritability
- Muscle tension
Desired Outcomes
- Patient appears approprately relaxed.
- Patient maintains focus, tuning out extraneous distractions.
- Patient verbalizes understanding of need for increased level of activity.
| Nursing Interventions | Rationale |
|---|---|
| Examine environment for factors causing sensory overload. | Determines factors, which may or may not be controllable. Cesarean birth requires many medical and nursing activities needed to ensure the health of mother and infant. Patient tends to concentrate on the procedures being performed and the conversations going on in the room. The birth experience may be compromised by invasive technology, tending to shift the focus from the birth of the infant to the surgical procedure. |
| Give information about the surgical routine, including sounds, lights, dress, and instruments. | Information about procedures, instruments, and alarms can help decrease anxiety, puts perceived “chaos” in perspective. |
| Decrease noise levels, limit conversations, and use equipment or alarms judiciously. | Patient may be keenly aware of sounds. Conversation, noise from equipment, and alarms may confuse patient or cause unnecessary anxiety. |
| Keep eye contact, especially when wearing mask. | Recognizes presence of patient or couple, conveys feeling of caring. |
| Incorporate patient or couple in operating room conversation or silence, using concerned communication. | Overlooking the patient can develop fear, which detracts from a positive birth experience. |
| Consider eliminating additional personnel from the scene. | Avoids interruption into personal space, which could increase anxiety. Individuals who are not required in care of the patient may detract from the intimacy of the birth experience. |
Deficient Knowledge
Deficient Knowledge: Absence or deficiency of cognitive information related to specific topic.
May be related to
- Lack of information
- Unfamiliarity with condition
- Misinterpretation
Possibly evidenced by
- Demand for information
- Narrative misconception
- False behaviors
Desired Outcomes
- Patient verbalizes understanding of indications for cesarean birth.
- Patient recognizes this as an alternative childbirth procedure to achieve the best result possible in the end.
| Nursing Interventions | Rationale |
|---|---|
| Appraise knowledge toward the procedure. | Most patients fail to retain the information instilled during childbirth classes. Therefore, patients have difficulty to remember or understand the details during the entire process. |
| Check on the level of stress and weather procedure was planned or not. | Defines patient’s or couple’s readiness to incorporate information. |
| Give accurate information in easy-to-understand terms and clarify misconceptions. | Stress of the situation can affect the patient’s ability to understand information required to make informed decisions. |
| Encourage couple to ask questions and verbalize their understanding on the matter. | This provides an opportunity to assess and evaluate patient’s or couple’s understanding of the situation. |
| Review indications necessitating alternative birth method. | Cesarean birth should be viewed as an alternative and not an abnormal situation to enhance the maternal and fetal safety and well-being. |
| Explain preoperative procedures in advance, and present rationale as appropriate. | Explanation of the logical reasons why a particular choice was made is vital in preparation for the procedure. |
| Educate patient postoperatively; including demonstration of leg exercises, proper coughing and deep breathing techniques, splinting, and abdominal tightening exercises. | Provides routine to prevent complications associated with venous stasis and hypostatic pneumonia, and to lessen stress on the operative site. Abdominal tightening reduces distress associated with gas formation and abdominal distension. |
| Further stress anticipated sensations during delivery and recovery period. | Having knowledge about the possible outcomes helps prevent unnecessary anxiety. |
Anxiety
Anxiety: Vague uneasy feeling of discomfort or dread accompanied by an autonomic response.
May be related to
- Perceived/Actual threat of maternal and fetal well-being
- Situational crisis
- Threat to self-concept
- Interpersonal transmission
Possibly evidenced by
- Apprehension
- Distress
- Feelings of inadequacy
- Increased tension
- Restlessness
- Sympathetic stimulation
Desired Outcomes
- Patient discusses feelings about cesarean birth.
- Patient appears relaxed and comfortable.
- Patient verbalizes fears for the safety of herself and infant.
| Nursing Interventions | Rationale |
|---|---|
| Assess psychological response to event and availability of support systems. | The greater the patient perceives the threat, the greater the level of her anxiety. |
| Consider cultural influences or expectations. | Some cultures (e.g., Latin, Mexican/Arab-American) may view surgical intervention as detrimental to the patient’s well-being or may believe patient will be stigmatized as a “weak woman” (e.g., Puerto Rican). |
| Know whether procedure is planned or not. | If the procedure is unplanned, patient or couple usually has no time for physiological or psychological preparation. Cesarean birth can still create apprehension even if it is planned due to perceived physical threat to the mother and infant. |
| Remain with the patient, and stay calm. Speak in a slow manner. Convey empathy. | Helps to reduce interpersonal transmission anxiety, and shows caring for the patient or couple. |
| Reinforce positive aspects of maternal and fetal condition. | Focuses on likelihood of desirable outcome and helps to bring perceived or actual threat into perspective. |
| Let the patient or couple verbalize or express inner thoughts and feelings. | Helps to distinguish negative feelings and concerns as well as provides chance to cope with uncertain or unresolved feelings or grief. The patient may also feel an emotional intimidation to her self-esteem, owing to her feelings that she has failed, that she is weak as a woman, and that her expectations have not been met. Partner may question own abilities in assisting patient and providing needed support. |
| Support/redirect expressed coping mechanisms. | Improves fundamental and automatic coping mechanisms, increases self-confidence and acceptance, and reduces anxiety. Note: Some actions by the patient may be viewed as ineffective (e.g., screaming and throwing things) and need to be redirected to enhance patient’s sense of control. |
| Allow patient to discuss and elaborate past childbirth experience or expectations, as appropriate. | Patient may have twisted thoughts of past delivery or unrealistic perceptions of abnormality of cesarean birth that will increase anxiety. |
| Allot time for privacy. | Allows patient or couple to internalize information, organize resources, and cope effectively. |
Risk for Situational Low Self-Esteem
Risk for Situational Low Self-Esteem: At risk for developing negative perception of self-worth in response to a current situation.
Risk factors may include
- Perceived “failure” at a life event
Possibly evidenced by
- [Not applicable; presence of signs/symptoms establishes an
actual diagnosis]
Desired Outcomes
- Patient identifies and discusses negative feelings.
- Patient verbalizes confidence in herself and in her abilities.
| Nursing Interventions | Rationale |
|---|---|
| Ascertain patient’s unusual feelings about self and pregnancy. Note cultural influences. | Diagnosis of a shift in self-concept is based on knowledge of past perceptions and experiences. Cesarean birth, even if planned or not, has the potential to change the way the patient feels about herself. The patient sees that the birth plan has been changed and that surgical intervention is needed to deliver the infant, while most women are able to deliver without any such intervention. |
| Allow the patient to verbalize feelings and thoughts. | Determines areas to be discussed. Patients’ feedback vary and may be hard to diagnose in the preoperative stage. Feelings of negative self-image related to disappointment in the birth experience may interfere with postpartal activities related to successful breastfeeding and infant care. |
| Encourage questions and give facts. Reinforce previous learning. | Improves understanding and clarifies misconceptions. |
| Associate cesarean birth as an alternative method of childbirth. | Terms like “C-section” and “normal delivery” may bolster patient’s thought that the cesarean birth is unusual and abnormal, and patient may look at self as inadequate, flawed or weak. |
| Provide verbal communication of assessment and interventions. Written information can be given at a later time. | When a problem of self-esteem arises for the patient, it may become more critical in the postpartal period. During the preoperative period, patient is focusing on the here and now and may not be ready to read or deal with additional information. |
| Recognize other couples or resources to be referred situation to after delivery. | At this significant time, the view of the situation usually does not provide chance to communicate with others who have shared the same experience. However, these activities may be beneficial in the future to help with resolution of feelings and perceptions. |
| Allow partner’s presence at the delivery as desired. | Provides support for the patient, encourages parental bonding, and gives additional input to the patient’s recall of the birth experience because memory lapses are more common during periods of crisis. Note: Cultural expectations may prevent support of father in birth process, necessitating attendance by a female family member. |
| Encourage the patient or couple to participate in room bonding activities (e.g., breastfeeding and holding the infant) as able. | Provides reinforcement of the birth experience and deemphasizes the surgical nature of the delivery. |
Powerlessness
Powerlessness: The lived experience of lack of control over a situation, including a perception that one’s actions do not significantly affect an outcome.
May be related to
- Interpersonal interaction
- Perception of illness-related regimen
- Lifestyle of helplessness
Possibly evidenced by
- Lack of participation in care of decision-making
- Passivity
- Verbalization of lack of control
Desired Outcomes
- Patient verbalizes fears and feelings of vulnerability.
- Patient expresses individual needs and desires.
- Patient participates in decision-making process whenever possible.
| Nursing Interventions | Rationale |
|---|---|
| Appraise circumstances contributing to sense of powerlessness. | Powerlessness becomes a major stress factor for patients experiencing their first hospitalization, which includes fear of the unknown. Unplanned (and sometimes planned) cesarean birth may be characterized by the patient’s or couple’s sense of loss of control over the birth experience. |
| Consider options in care when possible (e.g., IV placement, choice of anesthesia, and use of mirror) | Allows the patient to have some sense of control over the situation. |
| Recognize patient’s or couples expectations and desires concerning the delivery experience. | Provides opportunity to accommodate needs and encourage positive experience. |
| Allot personal time and space for the couple before the surgery, if possible. Stay with patient if partner is absent. | Lets the couple talk about the situation by themselves. Leaving patient alone may result in feelings of abandonment and adds anxiety. |
| Provide information, and talk about the patient or couple’s perceptions. | Lessens stress brought by misconceptions and unfounded fear |