Oops! You got it wrong...
EXPLANATION
✔Correct answer:
The mother may develop physiologic anemia due to the need for increased red blood cell mass, while the fetus requires about 350-400 mg of iron for growth. During pregnancy, a woman's body undergoes significant changes, including an increase in blood volume by about 30-50% to support the growing fetus. This increase in blood volume requires the production of more red blood cells (RBCs) to ensure adequate oxygen delivery to both the mother and the fetus. Iron is a critical component of hemoglobin, the protein in red blood cells that carries oxygen.
To meet the increased demand for RBC production, pregnant women require more iron. Additionally, the developing fetus needs approximately 350-400 mg of iron for its own growth and development, particularly in the formation of its own red blood cells and iron stores. If the mother's iron intake is insufficient, she may develop physiologic anemia, a common condition during pregnancy where the hemoglobin concentration decreases due to the dilution effect of the increased plasma volume.
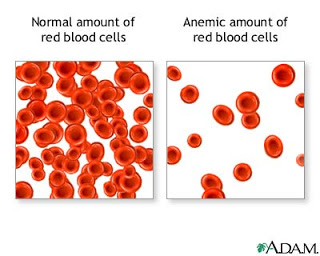
Physiologic anemia of pregnancy, also known as dilutional anemia, occurs because the plasma volume increases more than the red blood cell mass during pregnancy. This leads to a relative decrease in hemoglobin concentration and hematocrit. While the total RBC mass does increase, the expansion of plasma volume causes the blood to be more dilute. Iron is vital for the production of hemoglobin, and without adequate iron, the body cannot produce enough healthy red blood cells, leading to anemia. This can result in symptoms such as fatigue, weakness, and shortness of breath, which are commonly experienced by pregnant women with iron deficiency.
Think of iron as the building blocks needed to construct a house (red blood cells). During pregnancy, you're building a larger house because you're not only constructing it for yourself but also for the baby (increased RBC mass and fetal iron needs). If you don't have enough building blocks (iron), the construction slows down, leading to an incomplete or weaker structure (anemia).
Nurse Jenna should emphasize the importance of adequate iron intake during pregnancy, which can be achieved through diet and supplementation. Foods rich in iron, such as red meat, poultry, fish, legumes, and fortified cereals, should be recommended. Additionally, Nurse Jenna should inform the patient that vitamin C enhances iron absorption and suggest taking iron supplements with a source of vitamin C, such as orange juice. She should also educate the patient about possible side effects of iron supplements, such as constipation, and offer strategies to manage these effects.
- Encourage a balanced diet rich in iron-containing foods.
- Discuss the benefits of taking prenatal vitamins with iron and ensure they are taken as prescribed.
- Recommend taking iron supplements with vitamin C to enhance absorption.
- Provide guidance on managing side effects of iron supplements, like constipation, by increasing fiber intake and fluid consumption.
- Educate the patient about recognizing signs of anemia and when to report them to a healthcare provider.
✘Incorrect answer options:
The mother might experience anemia because of a reduced appetite. While reduced appetite can contribute to inadequate nutritional intake, it is not the primary reason for the increased need for iron during pregnancy. The key factor is the physiological changes in blood volume and the iron requirements of the growing fetus.
The fetus requires more red blood cells, which the mother needs to provide. While the fetus does require iron to produce its own red blood cells, the mother does not directly provide red blood cells to the fetus. Instead, the mother provides iron, which the fetus uses to build its own red blood cells.
The mother may have digestion issues due to pica. Pica, the craving for non-food substances, can lead to nutritional deficiencies, including iron deficiency, but it is not a primary reason for the increased iron requirement during pregnancy. The increased need for iron is due to the physiological demands of pregnancy, not digestive issues related to pica.
References
- Lowdermilk, D. L., Perry, S. E., Cashion, K., & Alden, K. R. (2019). Maternity and Women's Health Care. Elsevier.
- Cunningham, F. G., Leveno, K. J., Bloom, S. L., Spong, C. Y., & Dashe, J. S. (2018). Williams Obstetrics. McGraw-Hill Education.