Notes

Description
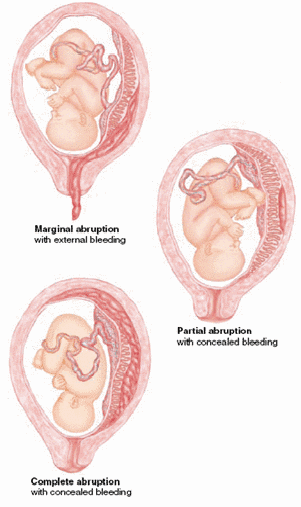
- Abruptio placenta is premature separation of a normally implanted placenta after the 20th week of pregnancy, typically with severe hemorrhage.
Etiology
- The cause of abruptio placenta is unknown.
- Risk factors include:
- Uterine anomalies
- Multiparity
- Preeclampsia
- Previous cesarean delivery
- Renal or vascular disease
- Trauma to the abdomen
- Previous third trimester bleeding
- Abnormally large placenta
- Short umbilical cord
Pathophysiology
- The placenta detaches in whole or in par from the implantation site. This occurs in the area of the deciduas basalis.
Assessment Findings
- Associated findings. Severe abruption placentae may produce such complications as:
- Renal failure
- Disseminated intravascular coagulation
- Maternal and fetal death
- Common clinical manifestation include:
- Intense, localized uterine pain, with or without vaginal bleeding.
- Concealed or external dark red bleeding
- Uterus firm to boardlike, with severe continuous pain
- Uterine contractions
- Uterine outline possibly enlarged or changing shape
- FHR present or absent.
- Fetal presenting part may be engaged.
- Laboratory and diagnostic study findings.
- Ultrasound may be able to identify the extent of abruption. However, the absence of an ultrasound finding does not rule out the presence of abruption.
Nursing Management
- Continuously evaluate maternal and fetal physiologic status, particularly:
- Vital signs
- Bleeding
- Electronic fetal and maternal monitoring tracings
- Signs of shock-rapid pulse, pallor, cold and most skin, decrease in blood pressure
- Decreasing urine output
- Never perform a vaginal or rectal examination or take any action that would stimulate uterine activity.
- Assess the need for immediate delivery. If the client is in active labor and bleeding cannot be stopped with bed rest, emergency cesarean delivery may be indicated.
- Provide appropriate management.
- On admission, place the woman on bed rest in a lateral position to prevent pressure on the vena cava.
- Insert a large gauge intravenous catheter into a large vein for fluid replacement. Obtain a blood sample for fibrinogen level.
- Monitor the FHR externally and measure maternal vital signs every 5 to 15 minutes. Administer oxygen to the mother by mask.
- Prepare for cesarean section, which is the method of choice for the birth.
- Provide client and family teaching.
- Address emotional and psychosocial needs. Outcome for the mother and fetus depends on the extent of the separation, amount of fetal hypoxia, and amount of bleeding.
Exam
Nursing Care Plan
Ineffective Tissue Perfusion
Related to:
- Excessive blood loss
Possibly evidenced by:
- Loss of blood
- FHR pattern
- Altered BP compared to baseline
- Altered PR Severe abdominal pain and rigidity
- Pallor
- Changes in LOC
- Decrease urine output
- Edema
- Delay in wound healing
- Positive Homan’s sign
- Skin temperature changes
Desired outcome:
| Nursing Interventions | Rationale |
|---|---|
| Assess patient’s vital signs, O2 saturation, and skin color. | For baseline data. |
| Monitor for restlessness, anxiety, hunger and changes in LOC | These conditions may indicate decreased cerebral perfusion |
| Monitor accurately I&O | To obtain data about renal perfusion and function and the extent of blood loss. |
| Monitor FHT continuously | To provide information regarding fetal distress and/or worsening of condition |
| Assess uterine irritability, abdominal pain and rigidity. | To determine the severity of the placental abruptio and bleeding |
| Assess skin color, temperature, moisture, turgor, capillary refill | To determine peripheral tissue perfusion like hypervolemia. |
| Elevate extremity above the level of the heart | Helps promote circulation. |
| Teach patient not to apply uterine pressure | Uterine pressure can cause pooling of venous blood in lower extremities |
| Instruct patient and/or SO to report immediately signs and symptoms of thrombosis: (1) pain in leg, groin (2) unilateral leg swelling (3) pale skin | To immediately provide additional interventions |
Risk for Shock
Related to:
- Significant blood loss of about 10% of the blood volume
- Separation of the placenta
- External or internal bleeding
Possibly evidenced by:
- Vaginal bleeding
- Couvelaire uterus or a tense and rigid uterus
- Increased pulse rate
- Decreased blood pressure
- Increased respiratory rate
- Decreased central venous pressure
- Decreased urine output
- Decreasing level of consciousness
- Cold, clammy skin
- Fetal bradycardia
Desired outcomes:
- Patient will display hemodynamic stability.
- Patient will regain vital signs within the normal range.
- Patient will be able to verbalize understanding of disease process, risk factors, and treatment plan.
- Patient will display a normal central venous pressure.
- Patient’s skin is warm and dry.
- Fetal heart rate is within normal range.
- Patient will exhibit an adequate amount of urine output with normal specific gravity.
- Patient will display the usual level of mentation.
| Nursing Interventions | Rationale |
|---|---|
| Assess for history or presence of conditions leading to hypovolemic shock. | The condition may deplete the body’s circulating blood volume and the ability to maintain organ perfusion and function. |
| Monitor for persistent or heavy fluid or blood loss. | The amount of fluid or blood loss must be noted to determine the extent of shock. |
| Assess vital signs and tissue and organ perfusion. | For changes associated with shock states |
| Review laboratory data. | To identify potential sources of shock and degree of organ involvement. |
| Collaborate in prompt treatment of underlying conditions and prepare for or assist with medical and surgical interventions. | To maximize systemic circulation and tissue and organ perfusion. |
| Administer oxygen by appropriate route. | To maximize oxygenation of tissues. |
| Administer blood or blood products as indicated. | To rapidly restore or sustain circulating volume and electrolyte balance. |
| Monitor uterine contractions and fetal heart rate by external monitor. | Assesses whether labor is present and fetal status; external system avoids cervical trauma. |
| Withhold oral fluid. | Anticipates need for emergency surgery. |
| Measure intake and output. | Enables assessment of renal function. |
| Measure maternal blood loss by weighing perineal pads and save any tissue that has passed. | Provides objective evidence of amount bleeding. |
| Maintain a positive attitude about fetal outcome. | Supports mother-child bonding. |
| Provide emotional support to the woman and her support person. | Assists problem solving which is lessened by poor self-esteem. |
Acute Pain
Related to:
- Sudden separation of placenta from the uterine wall
- Pain accompanying labor contractions during initial separation
Possibly evidenced by:
- Sharp, stabbing pain high in the uterine fundus
- Uterine tenderness
Desired outcomes:
- Patient will report relief or control of pain.
- Patient will follow prescribed pharmacological regimen.
- Patient will verbalize non pharmacological methods that provide relief.
- Patient will demonstrate use of relaxation skills and diversional activities as indicated.
| Nursing Interventions | Rationale |
|---|---|
| Assess for referred pain as appropriate. | To help determine the possibility of underlying condition or organ dysfunction requiring treatment. |
| Note client’s locus of control. | Individuals with external locus of control may take little or no responsibility for pain management. |
| Note and investigate changes from previous reports of pain. | To rule out worsening of underlying condition or development of complications. |
| Acknowledge the client’s description of pain and convey acceptance of client’s response to pain. | Pain is a subjective experience and cannot be felt by others. |
| Monitor skin color and temperature and vital signs. | These are usually altered in acute pain. |
| Note when pain occurs. | To medicate as appropriate. |
| Provide comfort measures, quiet environment, and calm activities. | To promote non pharmacological pain management. |
| Administer analgesics as indicated. | To maintain an acceptable level of pain. |
| Encourage adequate rest periods. | To prevent fatigue. |