Definition
- These are indices of health, or signposts in determining client’s condition. This is also known as cardinal signs and it includes body temperature, pulse, respirations, and blood pressure. These signs have to be looked at in total, to monitor the functions of the body.
Different considerations in taking Vital signs
- The frequency of taking TPR and BP depends upon the condition of the client and the policy of the institution.
- The procedure should be explained to the client before taking his TPR and BP.
- Obtain baseline data.
Vital Signs or Cardinal Signs are:
- Body temperature
- Pulse
- Respiration
- Blood pressure
- Pain
Body Temperature
- The balance between the heat produced by the body and the heat loss from the body.
Types of Body Temperature
- Core temperature –temperature of the deep tissues of the body.
- Surface body temperature
Alteration in body Temperature
- Pyrexia – Body temperature above normal range( hyperthermia)
- Hyperpyrexia – Very high fever, 41ºC(105.8 F) and above
- Hypothermia – Subnormal temperature.
Normal Adult Temperature Ranges
- Oral 36.5 –37.5 ºC
- Axillary 35.8 – 37.0 ºC
- Rectal 37.0 – 38.1 ºC
- Tympanic 36.8 – 37.9ºC
Methods of Temperature-Taking
I. Oral – most accessible and convenient method.
- Put on gloves, and position the tip of the thermometer under the patients tongue on either of the frenulun as far back as possible. It promotes contact to the superficial blood vessels and ensures a more accurate reading.
- Wash thermometer before use.
- Take oral temp 2-3 minutes.
- Allow 15 min to elapse between client’s food intakes of hot or cold food, smoking.
- Instruct the patient to close his lips but not to bite down with his teeth to avoid breaking the thermometer in his mouth.
Contraindications
- Young children an infant
- Patients who are unconscious or disoriented
- Who must breathe through the mouth
- Seizure prone
- Patient with N/V
- Patients with oral lesions/surgeries
II. Rectal- most accurate measurement of temperature
- Position- lateral position with his top legs flexed and drapes him to provide privacy.
- Squeeze the lubricant onto a facial tissue to avoid contaminating the lubricant supply.
- Insert thermometer by 0.5 – 1.5 inches
- Hold in place in 2minutes
- Do not force to insert the thermometer
Contraindications
- Patient with diarrhea
- Recent rectal or prostatic surgery or injury because it may injure inflamed tissue
- Recent myocardial infarction
- Patient post head injury
III. Axillary – safest and non-invasive
- Pat the axilla dry
- Ask the patient to reach across his chest and grasp his opposite shoulder. This promote skin contact with the thermometer
- Hold it in place for 9 minutes because the thermometer isn’t close in a body cavity
Note:
- Use the same thermometer for repeat temperature taking to ensure more consistent result
- Store chemical-dot thermometer in a cool area because exposure to heat activates the dye dots.
IV. Tympanic thermometer
- Make sure the lens under the probe is clean and shiny
- Stabilized the patient’s head; gently pull the ear straight back (for children up to age 1) or up and back (for children 1 and older to adults)
- Insert the thermometer until the entire ear canal is sealed
- Place the activation button, and hold it in place for 1 second
V. Chemical-dot thermometer
- Leave the chemical-dot thermometer in place for 45 seconds
- Read the temperature as the last dye dot that has change color, or fired.
Factors that Affect Body Temperature
- Age
- The infant is greatly influenced by the temperature of the environment and must be protected from extreme changes. Children’s temperature continues to be more labile than those of adults until puberty. Elderly people are at risk of hypothermia for variety of reasons. Such as lack of central heating, inadequate diet, loss of subcutaneous fat, lack of activity, and reduced thermoregulatory efficiency.
- Diurnal variations (circadian rhythms)
- This refers to the sleep – wake rhythm of the body, a pattern that varies slightly from person to person. Body temperature normally changes throughout the day, varying as much as 1.0C between the early morning and the late afternoon.
- Exercise
- Hard work or strenuous exercise can increase body temperature
- Hormones
- Women usually experience more hormones fluctuations than men do. Progesterone secretion at the time of ovulation raises body temperature above basal temperature
- Stress
- Stimulation of SNS can increase the production of epinephrine and norepinephrine, thereby increasing metabolic activity and heat production
- Environment
- Extremes in environmental temperatures can affect a person’s temperature regulatory systems.
Nursing Interventions in Clients with Fever
- Monitor V.S
- Assess skin color and temperature
- Monitor WBC, Hct and other pertinent lab records
- Provide adequate foods and fluids.
- Promote rest
- Monitor I & O
- Provide TSB
- Provide dry clothing and linens
- Give antipyretic as ordered by MD
Heat – producing & Heat – losing Mechanisms
- Heat production: most body heat is produced by the oxidation of foods; the rate at which it is produced is called METABOLIC RATE.
Heat Loss:
- Radiation
- Conduction
- Convection
- Evaporation
Pre – optic area of the Hypothalamus
- Temperature regulator; thermostat
- Receives input from temp receptors in the skin & mucous membranes (peripheral thermoreceptors) & internal structures (central thermoreceptors)
* If blood temp increases, neurons of the pre – optic area fire nerve if it decreases.
Heat Promoting Centers
- Vasoconstriction
- =Less blood flow from the internal organs to the skin= less heat transfer from the internal organs to the skin= increases internal body temperature
- Sympathetic Stimulation
- = stimulation of sympathetic nerves leading to the adrenal medulla = secretes epinephrine & norepinephrine = Increases cellular metabolism = increases heat production
- Skeletal Muscles
- = stimulation of part of the brain that increases muscle tone (stretch reflex + contraction of muscles = SHIVERING) = heat production
- Thyroxine
- = increases metabolism = increase in body temperature
Body Temperature Abnormalities
- Fever/hyperthermia/hyperpyrexia
- An abnormally high temp mainly results from infection from bacteria (& their toxins) & viruses. (Stimulates prostaglandin secretion)
- Other causes: heart attacks, tumors, tissue destruction by x – ray, surgery or trauma & rxns to vaccines.
- Heat cramps and Heat exhaustion
- Due to fluid & electrolyte loss
- Heat Stroke
- Hypothermia
The Thermometer
- A glass clinical thermometer is most commonly used to measure body temperature.
It has 2 parts:
- Bulb– contains mercury which expands when exposed to heat & rise in the stem
- Stem – is calibrated in degrees of Celcius or Fahrenheit
Pulse
- This is a wave of blood created by contraction of the left ventricle of the heart. The heart is a pulsating pump, and the blood enters the arteries with each heartbeat, causing pressure pulses or pulse waves. Generally, the pulse wave represents the stroke volume and the compliance of the arteries.
- Stroke volume is the amount of blood that enters the arteries with each contraction in a healthy adult.
- Compliance of the arteries is their ability to contract and expand. When a person’s arteries lose their distensibility, greater pressure is required to pump the blood into the arteries.
- Peripheral pulse is the pulse located in the periphery of the body, for example in the foot, hand and neck. Apical pulse is a central pulse. It is located at the apex of the heart.
Normal Pulse rate
- 1 year 80-140 beats/min
- 2 years 80- 130 beats/min
- 6 years 75- 120 beats/min
- 10 years 60-90 beats/min
- Adult 60-100 beats/min
- Tachycardia – pulse rate of above 100 beats/min
- Bradycardia– pulse rate below 60 beats/min
- Irregular – uneven time interval between beats.
What you need:
- Watch with second hand
- Stethoscope (for apical pulse)
- Doppler ultrasound blood flow detector if necessary
Obtaining Radial Pulse
- Wash your hand and tell your client that you are going to take his pulse
- Place the client in sitting or supine position with his arm on his side or across his chest
- Gently press your index, middle, and ring fingers on the radial artery, inside the patient’s wrist.
- Excessive pressure may obstruct blood flow distal to the pulse site
- Counting for a full minute provides a more accurate picture of irregularities
Obtaining Pulse Using Doppler device
- Apply small amount of transmission gel to the ultrasound probe
- Position the probe on the skin directly over a selected artery
- Set the volume to the lowest setting
- To obtain best signals, put gel between the skin and the probe and tilt the probe 45 degrees from the artery.
- After you have measure the pulse rate, clean the probe with soft cloth soaked in antiseptic. Do not immerse the probe
Factors Affecting Pulse Rate
- Age
- As age increases, the pulse rate gradually decreases
- Sex
- After puberty, the average male’s pulse rate is slightly lower than the female’s.
- Exercise
- Pulse rate usually increases with activity
- Fever
- The pulse rate increases in response to the lowered blood pressure that results from peripheral vasodilation associated with elevated body temperature, and because of the increased metabolic rate.
- Medications
- Some medications decrease the pulse rate, and others increase it.
- Hemorrhage
- Loss of blood from the vascular system normally increases pulse rate.
- Stress
- In response to stress, sympathetic nervous stimulation increases the overall activity of the heart. Stress increases the rate as well as the force of the heartbeat.
- Position changes
- When a person assumes a sitting or standing position, blood usually pools in dependent vessels of the venous system. Pooling results in a transient decrease in the venous blood return to the heart and a subsequent reduction in blood pressure reduction in blood pressure and increase in the heart rate.
Characteristics of Normal Pulse
- Rate
- This is the number of pulse beats per minute (70 – 80 beats/min in the adult). An excessively fast heart rate (100 beats/min) is referred to as tachycardia. A heart rate in the adult of 60 beats/minute or less is called bradycardia.
- Pulse rhythm
- This is the pattern of the beats and the intervals between the beats. Equal time elapses between beats of a normal pulse. A pulse with an irregular rhythm is referred to as a dysrhythmia or arrhythmia. It may consist of random, irregular beats or a predictable pattern of irregular beats.
- Pulse volume
- This is also called the pulse strength or amplitude. It refers to the force of blood with each beat. It can range from absent to bounding. A normal pulse can be felt with moderate pressure of the fingers and can be obliterated with greater pressure. A forceful or full blood volume that is obliterated only with difficulty is called a full or bounding pulse. A pulse that is readily obliterated with pressure from the fingers is referred to as weak, feeble, or thready. A pulse volume is usually measured on a scale 0 to 3.
Pulse Sites
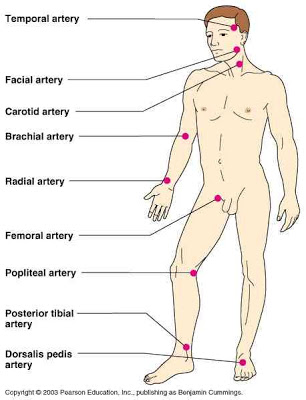
- Temporal, where the temporal artery passes over the temporal bone of the head. The site is superior and lateral to the eye.
- Carotid, at the side of the neck below the lobe of the ear, where the carotid artery runs between the trachea and the sternocleidomastoid muscle.
- Apical, at the apex of the heart.
- Brachial, at the inner aspect of the biceps muscle of the arm (especially in infants) or medially in the antecubital space (elbow crease).
- Radial, where the radial artery runs along the radial bone, on the thumb site of the inner aspect of the wrist.
- Femoral, where the femoral artery passes alongside the inguinal ligament.
- Popliteal, where the popliteal artery passes behind the knee. This point is difficult to find, but it can be palpated if the client flexes the knee slightly.
- Poserior tibial, on the medial surface of the ankle where the posterior tibial artery passes behind the medial malleolus.
- Pedal (dorsalis pedis), where the dorsalis pedis artery passes over the bones of the foot. This artery can be palpated by feeling the dorsum of the foot on the imaginary line drawn from the middle of the ankle to the space between the big and second toes.
Respiration
- Is the exchange of oxygen and carbon dioxide between the atmosphere and the body
Assessing Respiration
- Rate – Normal 14-20/ min in adult
- The best time to assess respiration is immediately after taking client’s pulse
- Count respiration for 60 second
- As you count the respiration, assess and record breath sound as stridor, wheezing, or stertor.
- Respiratory rates of less than 10 or more than 40 are usually considered abnormal and should be reported immediately to the physician.
- Resting respirations should be assessed when the client is at rest because exercise affects respirations, and increase their rate and depth as well. Respiration may also need to be assessed after exercise to identify the client’s tolerance to activity. Before assessing a client’s respirations, a nurse should be aware of:
- The client’s normal breathing pattern.
- The influence of the client’s health problems on respirations.
- Any medications or therapies that might affect respirations.
- The relationship of the client’s respirations to cardiovascular function.
Characteristics of Normal Respiration
- Respiratory rate
- This is described in breaths per minute. A healthy adult normally takes between 15 and 20 breaths per minute. Breathing that is normal in rate is eupnea. Abnormally slow respirations are referred to as bradypnea, and abnormally fast respirations are called tachypnea or polypnea.
- Depth
- This can be established by watching the movement of the chest. It is generally described as normal, deep, or shallow.
- Respiratory rhythm or pattern
- This refers to the regularity of the expirations and the inspirations. Normally, respirations are evenly spaced. Respiratory rhythm can be described as regular or irregular.
- Respiratory quality or character
- This refers to those aspects of breathing that are different from normal, effortless breathing. It includes:
-
- Amount of effort a client must exert to breathe. Usually, breathing does not require noticeable effort.
-
- The sound of breathing. Normal breathing is silent, but a number of abnormal sounds such as a wheeze are obvious to the nurse’s ear.
Blood Pressure
- This is the force exerted by the blood against a vessel wall. Arterial blood pressure is a measure of the pressure exerted by the blood as it flows through the arties. There are two blood pressure measures:
- Systolic pressure. This is the pressure of the blood because of contraction of the ventricles, which is the height of the blood wave.
- Diastolic pressure. This is the pressure when the ventricles are at rest. It is the lower pressure present at all times within the arteries.
- Pulse pressure is the difference between the diastolic and systolic pressures.
- Blood pressure is measured in millimeters of mercury (mm Hg) and recorded as a fraction. The systolic pressure is written over the diastolic pressure. The average blood pressure of a healthy adult is 120/80 mm Hg. A number of conditions are reflected by changes in blood pressure. The most common is hypertension, an abnormally high blood pressure. Hypotension is an abnormally low blood pressure below 100min Hg systolic.
Adult – 90- 132 systolic
60- 85 diastolic
Elderly– 140-160 systolic
70-90 diastolic
- Ensure that the client is rested
- Use appropriate size of BP cuff.
- If too tight and narrow- false high BP
- If too lose and wide-false low BP
- Position the patient on sitting or supine position
- Position the arm at the level of the heart, if the artery is below the heart level, you may get a false high reading
- Use the bell of the stethoscope since the blood pressure is a low frequency sound.
- If the client is crying or anxious, delay measuring his blood pressure to avoid false-high BP
Electronic Vital Sign Monitor
- An electronic vital signs monitor allows you to continually tract a patient’s vital sign without having to reapply a blood pressure cuff each time.
- Example: Dinamap VS monitor 8100
- Lightweight, battery operated and can be attached to an IV pole
- Before using the device, check the client7s pulse and BP manually using the same arm you’ll using for the monitor cuff.
- Compare the result with the initial reading from the monitor. If the results differ call the supply department or the manufacturer’s representative.
Physiology of Arterial Blood Pressure
- Pumping action of the heart
- Cardiac output is the volume of blood pumped into the arteries by the heart. When the pumping action of the heart is weak, less blood is pumped into arteries, and the blood pressure decreases. When the heart’s pumping action is strong and the volume of blood pumped into the circulation increases, the blood pressure increases. Cardiac output increases with fever and exercise.
- Peripheral Vascular Resistance
- This can increase blood pressure. The diastolic pressure is especially affected. The following are factors that create resistance in the arterial system:
-
- Size of the arterioles and capillaries. This determines in great part the peripheral resistance to the blood in the body pressure, whereas decreased vasoconstriction lowers the blood pressure.
-
- Compliance of the arteries. The arteries contain smooth muscles that permit them to contract, thus decreasing their compliance (distensibility). The major factor reducing arterial compliance is pathologic change affecting the arterial walls. The elastic and muscular tissues of the arteries are replaced with fibrous tissues. The condition, most common in middle-aged and elderly adults, is known as arteriosclerosis.
-
- Viscosity of the blood.
- Blood volume
- When the blood volume decreases, the blood pressure decreases because of decreased fluid in the arteries. Conversely, when the volume increase, the blood pressure increases because of the greater fluid volume within the circulatory system.
- Blood viscosity
- This is a physical property that results from friction of molecules in a fluid. The blood pressure is higher when the blood is highly viscous, that is, when the proportion of RBC’s to the blood plasma is high. This ratio is referred to as the hematocrit is more than 60 to 65%
Factors Affecting Blood Pressure
- Age. Newborn have a mean systolic pressure of 78mmHg. The pressure rises with age. The pressure rises with age, reaching a peak at the onset of puberty, and then tends to decline somewhat.
- Exercise. Physical activity increase both the cardiac output and hence the blood pressure. Thus, a rest of 20 to 30 minutes is indicated before the blood pressure can be readily assessed.
- Stress. Stimulation of the sympathetic nervous system increase cardiac output and vasoconstriction of the arterioles, thus increasing the blood pressure.
- Race. African – American males over 35 years have higher blood pressure than European – American males of the same age.
- Obesity. Pressure is generally higher in some overweight and obese people than in people of normal weight.
- Sex. After puberty, females usually have lower blood pressures than males of the same age; this difference is thought to be due to hormonal variations. After menopause, women generally have higher blood pressures than before.
- Medications. Many medications may increase or decrease the blood pressure; nurses should be aware of the specific medications a client is receiving and consider their possible impact when interpreting blood pressure readings.
- Diurnal variations. Pressure is usually lowest early in the morning, when the metabolic rate is lowest, then rises throughout the day and peaks in the late afternoon or early evening.
- Disease process. Any conditions affecting the cardiac output, viscosity, and or compliance of the arteries have a direct effect on the blood pressure.
Common Errors in Blood Pressure Assessment
|
Error
|
Effect |
| Bladder cuff too narrow | Erroneously high |
| Bladder cuff too wide | Erroneously high |
| Arm unsupported | Erroneously high |
| Insufficient rest before the assessment | Erroneously high |
| repeating assessment too quickly | Erroneously high |
| Cuff wrapped too loosely or unevenly | Erroneously high |
| Deflating cuff too quickly | Erroneously low systolic and high diastolic reading |
| Deflating cuff too slowly | Erroneously high diastolic reading |
| Failure to use the same arm consistently | Inconsistent measurements |
| Arm above level of the heart | Erroneously low |
| Assessing immediately after a meal or while client smokes | Erroneously high |
| Failure to identify auscultatory gap pressure | Erroneously low systolic pressure and erroneously low diastolic |
Auscultatory gap is the temporary disappearance of sounds normally heard over the brachial artery when the cuff pressure is high and the reappearance of the sounds at a lower level.
Provide excellent clues to the physiological functioning of the body.
- Alterations in body fxn are reflected in the body temp, pulse, respirations and blood pressure.
- These data provide part of the baseline info from which plan of care is developed.
- Any change from normal is considered to be an indication of the person’s state of health.
- Also called Cardinal Signs.
Pain
How to Assess Pain
- You must consider both the patient’s description and your observations on his behavioral responses.
- First, ask the client to rank his pain on a scale of 0-10, with 0 denoting lack of pain and 10 denoting the worst pain imaginable.
- Ask:
- Where is the pain located?
- How long does the pain last?
- How often does it occur?
- Can you describe the pain?
- What makes the pain worse?
- Observe the patient’s behavioral response to pain (body language, moaning, grimacing, withdrawal, crying,restlessness muscle twitching and immobility)
- Also note physiological response, which may be sympathetic or parasympathetic
Managing Pain
- Giving medication as per MD’s order
- Giving emotional support
- Performing comfort measures
- Use cognitive therapy